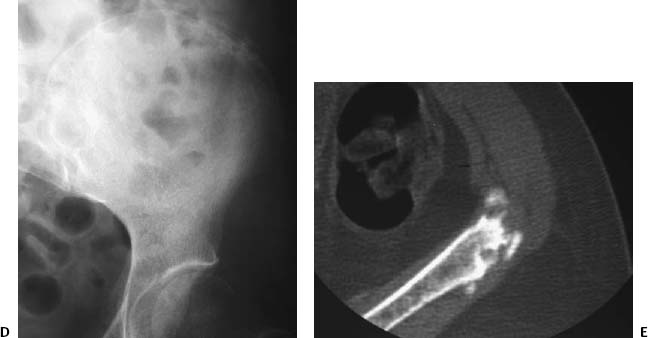
CASE 92 Anthony G. Ryan and Peter L. Munk A 20-year-old college football player presented with chronic anterior hip pain. Although he could recall no single acute event, there had been a period of intense preseason training 3 months previously. Figure 92A Figure 92B Radiograph of the left hip (Fig. 92A) reveals a thick, ossific, curvilinear density with smooth margins protruding from anterosuperior to the hip joint and projecting inferiorly. A CT scan (Fig. 92B) shows an irregularly marginated, heterogeneously ossified density immediately anterior to the anterior inferior iliac spine, with some associated irregularity of the underlying bone but no soft-tissue mass. Chronic avulsion fracture of the anterior inferior iliac spine, origin of the straight head of the rectus femoris muscle A differential diagnosis is inappropriate, as the history, location of the injury, and knowledge of the musculotendinous insertion anatomy yield the diagnosis. When excessive stress is applied to the “muscle-tendon-bone” unit, the weakest link in the chain will give way. The point of greatest vulnerability varies with age; in the child or adolescent, the weak point is at the physis until it undergoes bony fusion (early to mid 20s). Thus, when excessive strain is applied through a muscle onto a bone underlying, which is an apophysis, the muscle-tendon-bone complex will break at the apophysis, giving rise to a characteristic avulsion fracture. Although there is great variation in the spectrum of resultant avulsions, when typical, they pose no diagnostic dilemma. When their appearances are atypical, however, as they can be in the subacute or chronic states, they may mimic other, more aggressive lesions, such as neoplasms, or infection. Familiarity with the range of appearances of such lesions aids in the avoidance of inappropriate biopsy. Around the pelvis, the most common sites for these avulsions are, in order of decreasing frequency: The injuries may occur as a result of repetitive trauma or secondary to a single severe, usually eccentric, contraction during running, jumping, or kicking a ball, with subsequent healing of the acute fracture. The sports most commonly producing the injuries are soccer, gymnastics, football, baseball, hurdling, cheerleading, and track athletics (sprinting, jumping). Figure 92C Chronic avulsion of the right ischial tuberosity in a 22-year-old soccer player. Plain film shows a large fragment partially fused with the underlying ischium, the irregular junction line characterized by an intermittent sclerotic pattern, partial fusion posterosuperiorly, and a persistent lucent line at the fracture interface.
Chronic Avulsion Fractures
Clinical Presentation


Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


