CASE 93 Hema N. Choudur, Anthony G. Ryan, and Peter L. Munk An elderly woman sustained a fall when she inadvertently slipped on wet ground in her backyard. She was unable to pull herself up and was brought to the emergency department by her husband. On examination, she had pain and tenderness in her left groin and thigh and was unable to move her hip. The left lower limb was in external rotation. Her pulses and sensorimotor examination were normal. Figure 93A Figure 93B A plain radiograph (Fig. 93A) shows an impacted fracture of the left femoral neck. A CT scan (Fig. 93B) of the same patient delineates the undisplaced fracture line more clearly. Impacted fracture of the left midfemoral neck. Femoral neck fractures are very common and are associated with a high degree of morbidity and mortality; therefore, their diagnosis and treatment are of paramount importance. These fractures occur with a frequency of 1 in 1000 per year. One fourth of patients die within 6 months, and two thirds have persistent swelling and pain. Fewer than half return to preinjury level of function despite treatment. Whether a femoral neck fracture occurs or not depends on bone mineralization and the type of fall. Osteoporosis, osteomalacia, fatigue fractures, malignancy, and Paget’s disease are the most frequently encountered etiologies of femoral neck fractures. The length of the femoral neck and the absence of osteoarthritis also have an influence. For patients under the age of 55 years, femoral neck fractures are more common in men involved in road traffic accidents, but in patients over the age of 55, they are more common in women. After age 65, the increase is exponential in both sexes. These fractures are more common in Caucasian women than Black women. The two proposed mechanisms in older individuals are a fall, producing a direct blow on the greater trochanter, and lateral rotation of the lower limb. A large direct force on the femoral shaft with or without a rotational component can cause similar injuries in young adults. Even a minor trauma that goes unnoticed can cause a femoral neck fracture in an elderly osteoporotic woman. Osteopenia is by far the most common cause of femoral neck fractures, aside from Colles’ and proximal humeral fractures. Blood supply to the femoral head and neck involves two anastomotic rings: one extracapsular at the base of the neck, formed mainly by the medial and lateral circumflex femoral arteries posteroanteriorly, with contributions from the superior and inferior gluteal arteries, and the other a subsynovial intra-articular ring at the articular cartilage-neck junction formed by the retinacular arteries, which are branches of the ascending cervical arteries. The artery of the ligamentum teres in adults supplies only a small portion of the head, through its medial epiphyseal branches. The epiphysis is mainly supplied by the lateral and less so by the medial epiphyseal vessels and from the subsynovial ring. The metaphysis is supplied by the extracapsular ring, the ascending cervical arteries, and the subsynovial ring. Fracture may disrupt this blood supply. Because the head depends mainly on the retinacular vessels, avascular necrosis is an often-seen complication of femoral neck fractures. Inadequate reduction may also result in avascular necrosis from kinking or stretching of the supplying vessels. It is also important to note that the intracapsular neck does not heal by callus formation, as there is no cambium to its fibrous covering. Inability to bear weight in the absence of any known trauma should prompt a clinician to evaluate the proximal femur in the elderly, as trivial trauma can result in unrecognized fractures.
Hip Fractures
Clinical Presentation

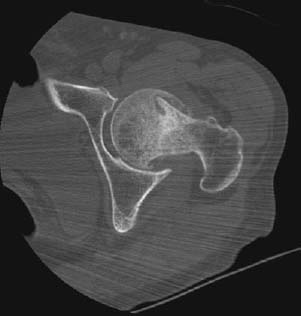
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


