with the imaging findings. False-positive and false-negative results are encountered in the evaluation of the acute abdomen. An imaging finding not commensurate with clinical presentation, physical exam, or laboratory studies must be viewed with some suspicion. Knowledge of detailed patient medical data facilitates the radiologist selecting the appropriate imaging modality and improves interpretation and detection of subtle diagnostic findings.
TABLE 14.1 Summary of American College of Radiology Appropriateness Criteria for Selected Gastrointestinal, Genitourinary, and Cardiovascular Conditions | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
This series of radiographs comprise the standard abdominal series.
TABLE 14.2 Recommended CT Techniques for Routine Abdomen and Pelvis Imaging | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
and a pitch of 1.0 to 1.5 is commonly used. Delayed scanning of the kidneys is performed for evaluation of renal excretion with helical axial imaging at 10 mm collimation.
protuberant abdomen, debilitated patients, or patients with little body fat.
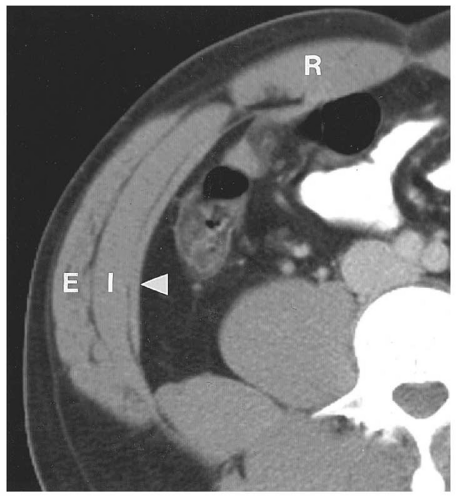 Figure 14.1. CT of the abdominal wall. CT image at the level of the upper portion of the umbilicus shows the muscles of the abdominal wall: external oblique (E), internal oblique (I), and transversus abdominis (arrowhead). The rectus abdominis muscle (R) is seen anteriorly closer to the midline. |
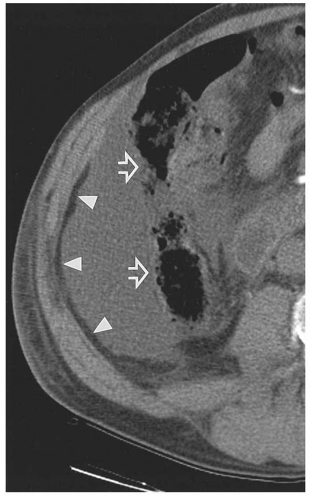 Figure 14.2. Fluid in the paracolic gutter. CT shows a collection of fluid in the right paracolic gutter displacing the ascending colon and hepatic flexure medially. The displacement is accentuated by the absence of the right kidney in this individual. The increased distance between the flank stripe (white arrowheads) and the lateral wall of the colon (open arrows) was evident on a conventional radiograph. |
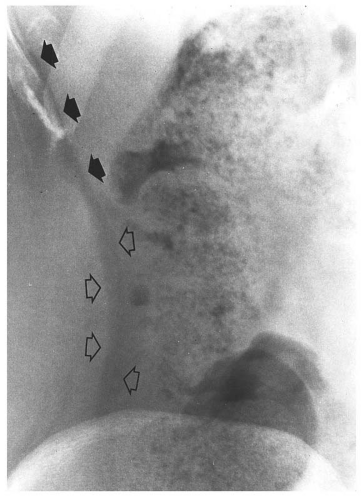 Figure 14.3. Radiographic appearance of the soft tissues of the right flank. The extraperitoneal fat (“flank stripe”) produces the sharply defined, gently curved lucent band (open arrows) extending from below the iliac crest to above the lateral margin of the liver (solid arrows). Gas and feces identify the ascending colon and the hepatic flexure and outline the inferior margin of the liver. |
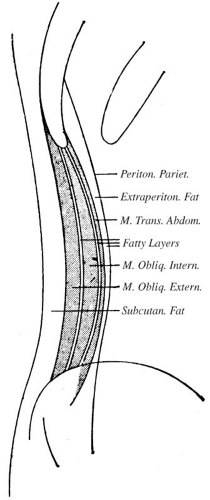 Figure 14.4. Schematic drawing of the soft tissues of the flank. The extraperitoneal (preperitoneal, properitoneal, and retroperitoneal) fat produces the lucent shadow of the flank stripe. (From Soyer P. Segmental anatomy of the liver: utility of a nomenclature accepted worldwide. Am J Roentgenol. 1993;161(3):572-573, with permission.) |
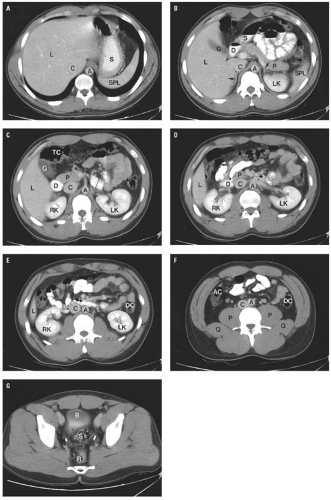 Figure 14.5. Normal CT anatomy. A: Diaphragmatic hiatus. Note the collapsed esophagus immediately anterior to the aorta. L, liver; C, inferior vena cava; A, aorta; S, stomach; SPL, spleen. B: The pancreatic body and tail are located immediately anterior to the splenic vein. Note the superior end of the gallbladder fossa, which is located immediately caudal to the interlobar fissure. An air-oral contrast material level is present in the second portion of the duodenum. Both adrenal glands are visible in this section (arrows). L, liver; G, gallbladder; D, duodenum; C, inferior vena cava; S, stomach; A, aorta; P, pancreatic tail; LK, left kidney; SPL, spleen. C: Pancreatic head. At the level of the superior mesenteric artery origin, an elongated but homogeneous pancreatic head has no contour abnormalities. The duodenum is filled with contrast material on this image. Note the close relationship between the hepatic flexure, the gallbladder, and the liver. L, liver; G, gallbladder; TC, transverse colon; D, duodenum; RK, right kidney; P, pancreatic head; C, inferior vena cava; S, stomach; A, aorta; LK, left kidney. D: The third portion of the duodenum. Note the contrast-filled duodenum crossing anterior to the inferior vena cava and the aorta immediately posterior to the superior mesenteric artery and vein at the upper end of the root of the small bowel mesentery. L, liver; RK, right kidney; D, duodenum; P, pancreatic head; C, inferior vena cava; A, aorta; LK, left kidney. E: Kidneys. Image at the level of the left splenic vein shows the inferior portion of the right lobe of the liver. The superior mesenteric vein and artery are visible in the root of the small bowel mesentery. L, liver; RK, right kidney; C, inferior vena cava; A, aorta; DC, descending colon; LK, left kidney. F: Paracolic gutters. In the normal individual, the paracolic gutter is a potential space between the parietal peritoneum of the body wall and the visceral peritoneum surrounding the ascending and descending colon. Note the multiple small arteries and veins coursing through the mesentery. AC, ascending colon; P, psoas muscle; Q, quadratus lumborum muscle; C, inferior vena cava; A, aorta; DC, descending colon. G: Peritoneal reflection. This image is below the anterior surface of the peritoneal reflection where the parietal peritoneum covers the dome of the bladder. B, bladder; S, sigmoid colon; R, rectum. |
is fat between other structures, the retroperitoneum also contains the great vessels, pancreas, portions of the duodenum and colon, the adrenal glands, kidneys, ureters, and bladder. The extraperitoneal spaces extend from the diaphragm to the floor of the pelvis and wrap around the entire peritoneal cavity. They are divided into the abdominal retroperitoneum, which is the subject of this section, and the pelvic perivesical space, which is described in conjunction with normal anatomy of the pelvis in Chapters 15 and 17.
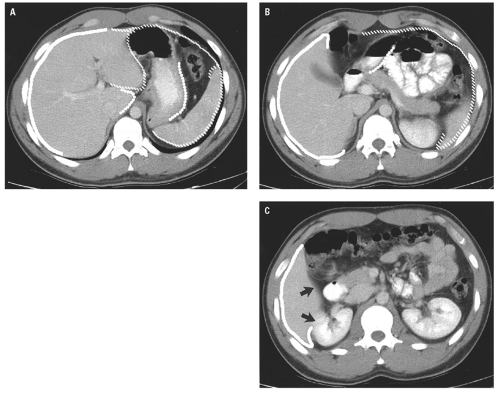 Figure 14.6. Peritoneal spaces. A: The heavy white line outlines the right perihepatic space. The hash marks outline the left peritoneal space, which is made up of the anterior left perihepatic space, the posterior left perihepatic space, and the perisplenic space. The series of dots outlines portions of the lesser sac around the caudate lobe and posterior to the stomach. B: At a lower level, the right perihepatic space, outlined by the heavy white line, is limited posteriorly by the coronary ligament, which defines the bare area of the liver. The left posterior hepatic space has ended below the liver. A small portion of the lesser sac is visible between the stomach and the pancreas. C: Caudally, the right perihepatic space continues as the hepatorenal recess (Morrison pouch) (arrows) between the liver and the right kidney. |
renal fascia and contains only fat. This space becomes important when inflammatory processes track into it.
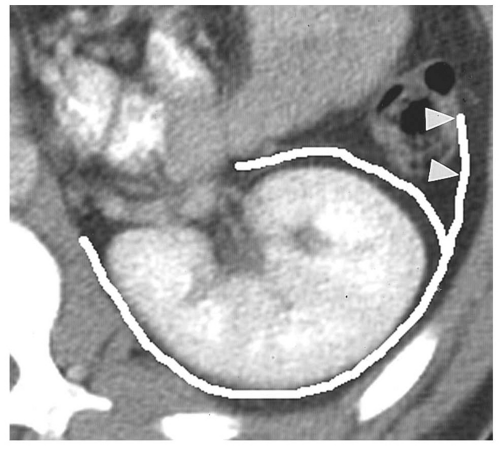 Figure 14.7. Perirenal space. The heavy white line outlines the renal fascia, which merges with the lateroconal fascia extending anteriorly to the descending colon (arrowheads). |
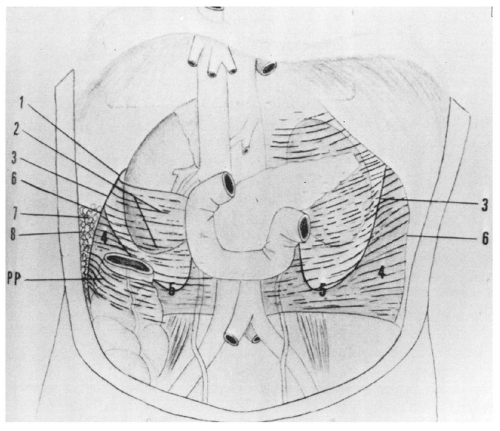 Figure 14.8. Schematic representation of the retroperitoneal compartments. This drawing clearly illustrates the conical configuration of the inferior portion of the perirenal space (5). Other extraperitoneal structures represented include the posterior renal fascia (1), anterior renal fascia (2), line of fusion of anterior and posterior renal fasciae (3), lateroconal fascia (4), line of fusion of lateroconal fascia with posterior parietal peritoneum (6), posterior pararenal fat extending into the flank stripe (7), transverse fascia (8), and parietal peritoneum (PP). (From Meyers MA, Whalen JP, Peelle K, et al. Radiologic features of extraperitoneal effusions. An anatomic approach. Radiology. 1972;104(2):249-257, with permission.) |
artery arises from the anterior surface of the aorta (Fig. 14.9C). One centimeter below this, the renal arteries arise from the lateral aspects of the aorta (Fig. 14.9D). Just above the aortic bifurcation, the small inferior mesenteric artery arises from the anterior wall of the aorta (Fig. 14.9E).
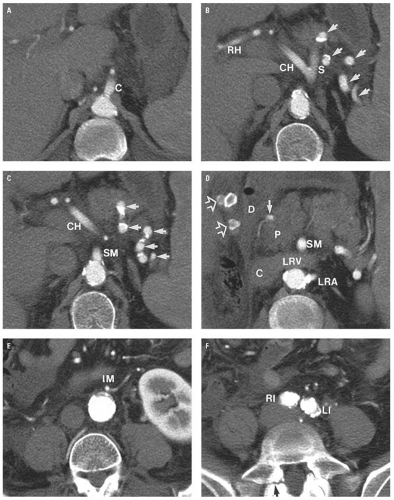 Figure 14.9. Abdominal vascular anatomy. A: Origin of the celiac axis (C) at the inferior margin of the diaphragmatic hiatus. B: Division of the celiac axis into common hepatic (CH) and splenic (S) arteries. Note the splenic artery coursing in and out of the plane of section (arrows). The right hepatic (RH) artery is visible in the porta hepatis. The third division of the celiac axis, the left gastric artery, is not visible on the section. C: Superior mesenteric (SM) artery origin 1.3 cm caudal to the celiac axis origin. The splenic artery is also visible (arrows).CH is the common hepatic artery. D: Origin of the left renal artery (LRA). The right kidney is absent. The superior mesenteric (SM) artery passes anterior to the left renal vein (LRV). The gastroduodenal artery (solid arrow) passes along the anterior margin of the pancreatic head. Several faceted rim-calcified gallstones (open arrows) are seen in the gallbladder. E: The inferior mesenteric (IM) artery originated from the anterior wall of the aorta on the image immediately cephalad to this one; on this image, the inferior mesenteric artery tracks to the left of midline. F: Aortic bifurcation at the L4-5 disc level. The irregularity of the common iliac artery walls and the aortic lumen is due to atherosclerosis. The aorta bifurcates into right (RI) and left (LI) common iliac arteries. There is a pars interarticularis defect on the right side of L5 (arrow). |
(Fig. 14.13A). Caudally, the common hepatic duct (CHD) is seen anterolateral to the main portal vein. The hepatic artery lies anteromedial to the main portal vein. In cross section, both the CHD and hepatic artery appear as small, round structures, anterior to the portal vein. On the transverse view, the appearance of the CHD, hepatic artery, and portal vein has been likened to Mickey Mouse (Fig. 14.13B) and provides a frame of reference for longitudinal imaging of the CHD and common bile duct. A long segment of the bile duct may be demonstrated longitudinally, anterior to the portal vein (Fig. 14.13C). A portion of the hepatic artery is often seen in cross section between the bile duct and the portal vein. The size of the CHD varies with age and increases slightly after cholecystectomy. Generally, 6 mm is taken as the upper limit of the normal diameter of the CHD in adults. In adults older than 75 years, 10 mm is the upper limit of normal, whereas in children, 3 mm is the upper limit of normal. Distally, the common bile duct shows even greater variability in caliber and may be up to 3 mm larger than the CHD.
TABLE 14.3 Couinaud-Bismuth Segments and Corresponding Liver Anatomy | ||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||
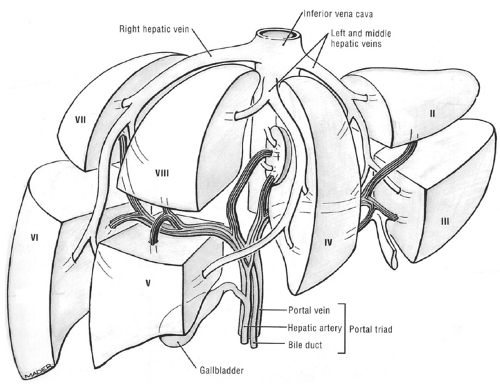 Figure 14.10. Segmental and vascular anatomy of the liver. Each segment of the liver is supplied by a branch of the hepatic artery, bile duct, and portal vein. The hepatic veins do not follow the structures of the portal triad and are considered intersegmental in that they drain portions of adjacent segments. (From Agur AMR. The abdomen. In: Grant’s Atlas of Anatomy. 9th ed. Baltimore, MD: Lippincott Williams & Wilkins; 1991:115, with permission.) |
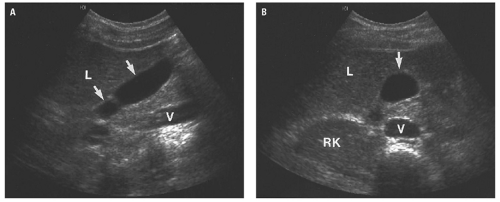 Figure 14.11. Normal gallbladder. Longitudinal (A) and transverse (B) ultrasound images of a normal gallbladder (arrows) within the gallbladder fossa immediately posterior to the liver (L). V, inferior vena cava; RK, right kidney. |
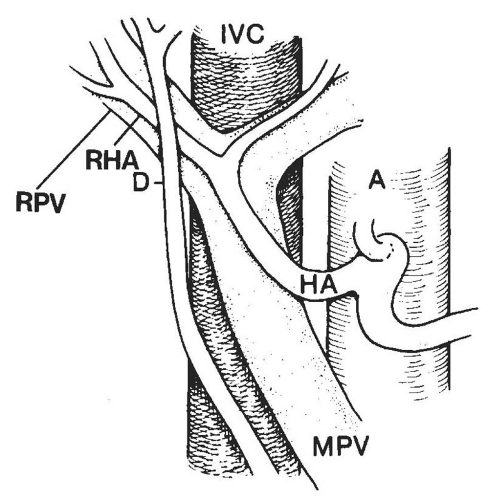 Figure 14.12. Schematic representation of the normal porta hepatis and their relationships to the inferior vena cava (IVC). The structures of the porta hepatis bear a constant relationship to each other. The common hepatic duct (D) lies lateral to the proper hepatic artery (HA) and crosses anterior to the right hepatic artery (RHA) and right portal vein (RPV). MPV, main portal vein; A, aorta. These relationships may be readily appreciated on both ultrasound and CT. (From Zeman RK, Simeone JF. The biliary ducts: anatomy, examination, technique and pathophysiologic considerations. In: Taveras JM, Ferrucci JT, eds. Radiology: Diagnosis, Imaging, Intervention. Vol 4. Philadelphia, PA: JB Lippincott; 1998:1-18. Modified from Zeman RK, Burrell MI. Gallbladder and Bile Duct Imaging: a Clinical Radiologic Approach. New York, NY: Churchill Livingstone; 1987, with permission. |
contrast material. CT usually demonstrates the common bile duct passing through the head of the pancreas.
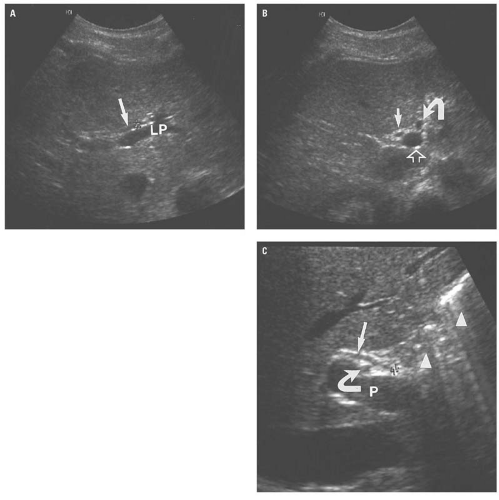 Figure 14.13. Ultrasound anatomy of the bile ducts. A: Transverse image through the porta hepatis at the left portal (LP) vein shows a normal caliber left hepatic duct (arrow) measuring 2 mm in diameter. Note that peripheral intrahepatic ducts are not visible. B: Transverse image through the porta hepatis as it exits the liver shows the “Mickey Mouse” appearance of the porta hepatis in a normal patient. The “head” is the portal vein (open arrow), the “right” (lateral) ear represents the common hepatic duct (straight arrow), and the “left” (medial) ear represents the hepatic artery (curved arrow). Use of these landmarks can help in tracing the common duct through the porta hepatis. C: Longitudinal image through the extrahepatic bile duct shows the common duct (electronic cursor and straight arrow) measuring 1 mm in diameter. The main portal vein (P) is located posterior to the common duct. The right hepatic artery (curved arrow) is visible between the common duct and the main portal vein. Note the “dirty shadows” from a bowel loop located posterior and inferior to the liver (arrowheads). |
 Figure 14.14. Early bolus effect in the spleen. CT image through the inferior portion of the spleen shows mottled central enhancement of the spleen with unenhancing parenchyma peripherally. This image was made 30 seconds after the beginning of the bolus of contrast material because of a technical error. |
in the caliber of the ureter through its course from the renal pelvis to the bladder.
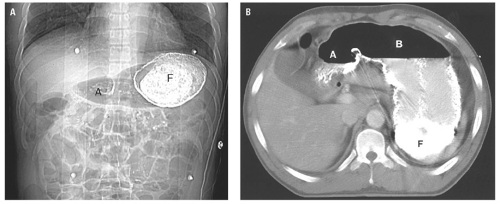 Figure 14.15. Stomach anatomy. A: Supine scout image for abdominal CT shows barium in the gastric fundus (F) and air in the gastric antrum (A). B: CT image through the stomach shows dense barium in the gastric fundus, barium mixed with gastric fluid in the dependent portion of the body, and air in the nondependent portion of the gastric body (B) and gastric antrum (A). |
of the passage of liquid contrast material. The appearance of the small bowel is variable and depends on the degree of distention by gas or contrast material. The normal, nondistended small bowel wall is thick, but when completely distended by gas or contrast material, the wall measures no more than 3 mm in thickness. The colon is usually not well distended, so wall thickness is difficult to assess; however, when distended, the colon wall is typically less than 3 mm thick.
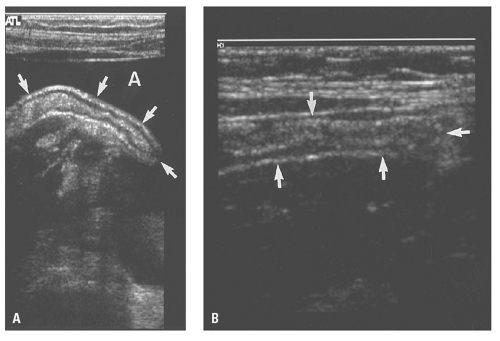 Figure 14.16. Ultrasound of the normal appendix. A: Longitudinal ultrasound image in a child with ascites (A) allows unusually clear visualization of the normal appendix (arrows). Note the echogenic submucosa, the hypoechoic muscularis, and echogenic serosa. B: Longitudinal ultrasound image of a normal appendix (arrows) in a child shows similar ultrasonographic features, but the surrounding echogenic abdominal wall makes the normal appendix more difficult to see. (Case courtesy of Cynthia I. Caskey, MD.) |
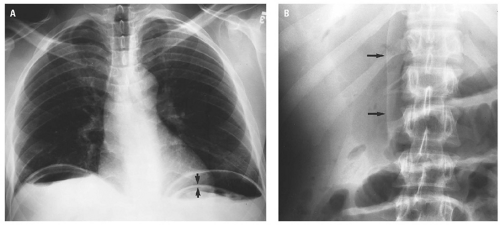 Figure 14.17. Pneumoperitoneum on erect radiograph. A: PA erect chest radiograph shows free intraperitoneal air beneath each hemidiaphragm. Note air outlining both sides of the stomach (arrows). B: In the same patient, the close-up view AP supine abdominal radiograph shows the falciform ligament (arrows) outlined by free air. |
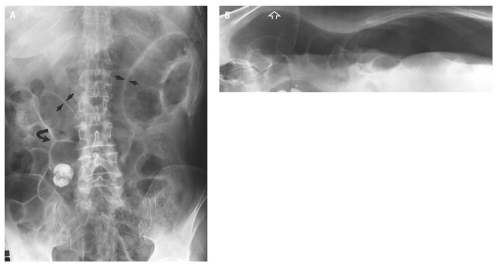 Figure 14.18. A: Supine view of the abdomen in a patient with massive pneumoperitoneum shows that both sides of several bowel loops are outlined by air in both the right and left upper quadrants (arrows). The triangular gas bubble between adjacent bowel loops (curved arrow) is Rigler triangle. This may be the only sign of a less extensive pneumoperitoneum. B: Right side up decubitus view of the abdomen shows the possible locations for free intraperitoneal air in the right perihepatic space and in the right side of the pelvis (open arrow). Note air outlining several small bowel loops and an air-ascites level within the peritoneal cavity. |
medial half of the right upper quadrant of the abdomen below the hemidiaphragm is the most frequent juxtahepatic pattern of pneumoperitoneum (Fig. 14.17B). Other right upper quadrant signs include visualization of the falciform ligament as a thin linear density over the liver (Figs. 14.17B and 14.20); air within the hepatorenal recess (Morrison pouch) (Fig. 14.19A); extraluminal air outlining the serosal surface of bowel loops (Rigler sign) (Fig. 14.18); and a large, lucent, oval air collection in the midabdomen (football sign) (Fig. 14.20).
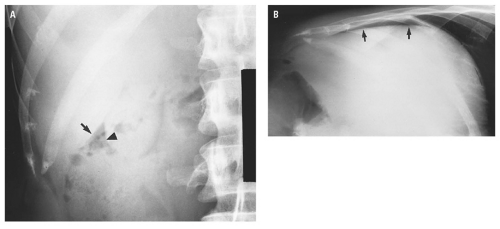 Figure 14.19. Pneumoperitoneum due to perforated duodenal ulcer. A: Supine radiograph shows free air between the liver edge (arrow) and the outer margin of the gallbladder fundus (arrowhead). B: Right side up decubitus radiograph shows free intraperitoneal air in the right perihepatic space (arrows). |
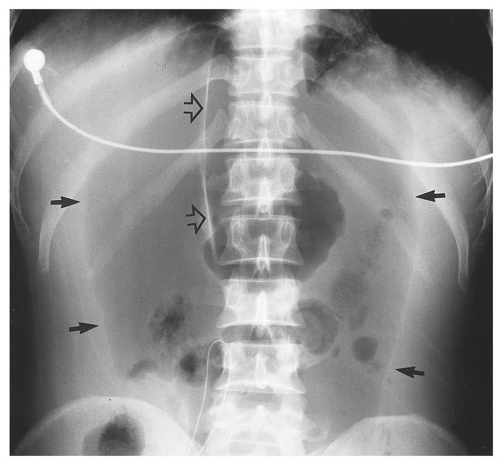 Figure 14.20. Massive pneumoperitoneum with demonstration of the falciform ligament (open arrows) outlined by air. The large collection of air in the midabdomen is described as a “football” sign (solid arrows). |
pouch. Findings can be subtle, with pneumoperitoneum manifesting as only a few trapped air bubbles in the mesentery. Wide window settings of more than 750 HU can help detect subtle air collections.
 Figure 14.21. Pneumoperitoneum on CT. CT image through the midabdomen displayed at lung windows shows a collection of free intraperitoneal air (arrow) under the anterior abdominal wall in the least dependent part of the abdomen. |
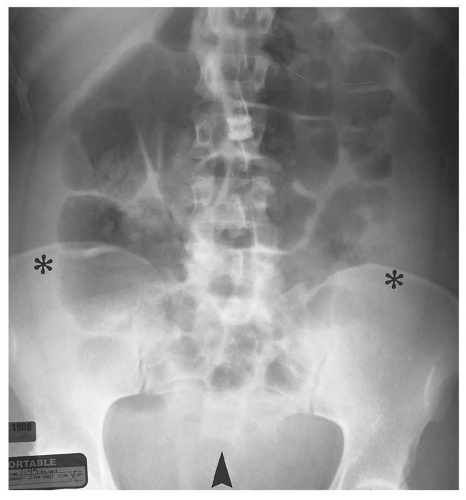 Figure 14.22. AP supine radiograph of the abdomen in a patient with ascites. Note the medial displacement of the air-filled loops of bowel including the ascending and descending colon, which are separated from the flank stripes by fluid in the paracolic gutters (asterisks). Airfilled loops of bowel have floated out of the fluid-filled pelvis (arrowhead). |
(Fig. 14.25). Extraperitoneal abscess of the psoas muscles conforms to the shape of the muscle but may cause mass effect on adjacent structures (Fig. 14.26). Abscesses contain fluid with low attenuation near that of water. One-third contain small air bubbles or air-fluid levels. An enhancing rim of granulation tissue is characteristic, particularly as the abscess matures, but is present in only a minority of cases. Thickening of fascial planes and soft tissue strands infiltrating fat adjacent to the abscess are signs of inflammation that help distinguish an abscess from sterile fluid collections. However, when the characteristic features of abscess are absent, aspiration may be required to establish the diagnosis.
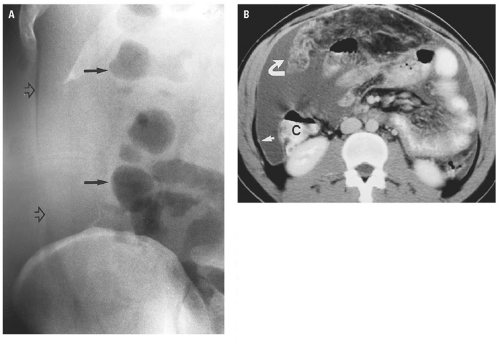 Figure 14.23. Ascites. A: Supine radiograph reveals increased opacity in the right paracolic gutter with increased distance between the flank stripe (open arrows) and the ascending colon (solid arrows). B: Enhanced CT at umbilicus reveals thickening of the mesentery and omentum (curved arrow). Ascites is present, displacing the ascending colon (C) from the abdominal wall, correlating with the appearance on the supine radiograph. The parietal peritoneum is thickened (straight arrow). |
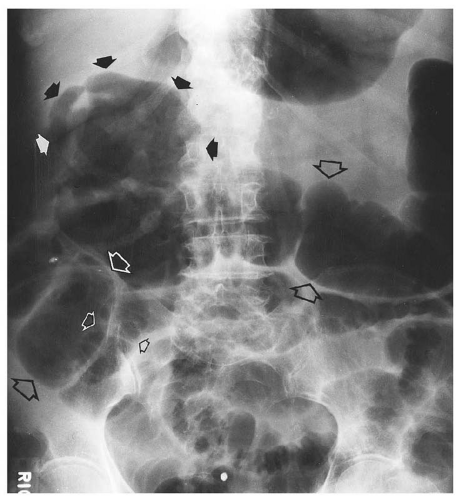 Figure 14.24. Subhepatic abscess. Solid arrows indicate a gas-filled subhepatic abscess. Large open arrows indicate distended colon. Small open arrows indicate dilated small intestine. The abscess produced peritonitis and resultant adynamic ileus. |
 Figure 14.25. Postsurgical perisplenic abscess. Enhanced CT image below the left splenic hilum shows a thick-walled fluid collection in the perisplenic space (asterisks). A smaller collection is seen anterior to the spleen (arrow). The 400 mL of purulent material was aspirated. |
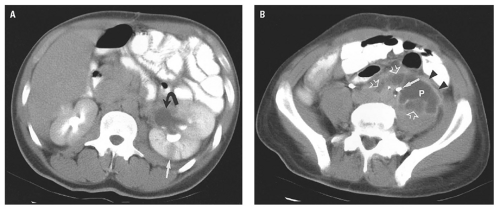 Figure 14.26. Left psoas abscess and left pyonephrosis. Young man with previous abdominal gunshot wound. A: Enhanced CT image through the left renal pelvis shows marked left hydronephrosis (curved arrow) and persistent nephrogram with focal hypoattenuation, indicating acute pyelonephritis (straight arrow). B: Image in the pelvis demonstrates a 5.1-by-3.3-cm left psoas abscess (P) with an enhancing wall displacing the left ureter medially. Note the enhanced rim of the abscess (arrowheads) and the small loculi posteriorly and medially (open arrows). Bullet fragments (arrow) are seen medial to the left ureter. |
material should be administered to provide additional information about the size and location of intraluminal thrombus and to demonstrate extravasation from a contained rupture (Fig. 14.29). CT is able to show the principal diagnostic sign of a ruptured AAA, a periaortic retroperitoneal hematoma, which may extend into the perirenal or pararenal spaces. In the absence of retroperitoneal hemorrhage, signs of impending rupture may be detected, including “hyperdense crescent” sign, a high-attenuation crescent within the wall of the aorta; focal contour bulge; increased size; or the
demonstration of a focal defect in an otherwise calcified aortic wall (Fig. 14.30).
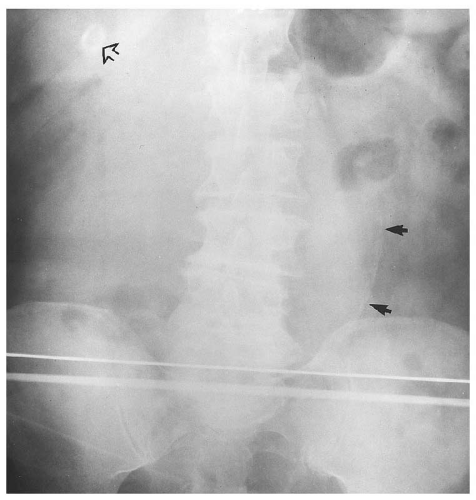 Figure 14.27. Ruptured abdominal aortic aneurysm (AAA). AP supine radiograph shows the atherosclerotic margin of a large AAA (arrows) in a patient presenting with an abdominal catastrophe. A rim-calcified gallstone is noted incidentally (open arrow). This radiograph does not depict the associated retroperitoneal hemorrhage. |
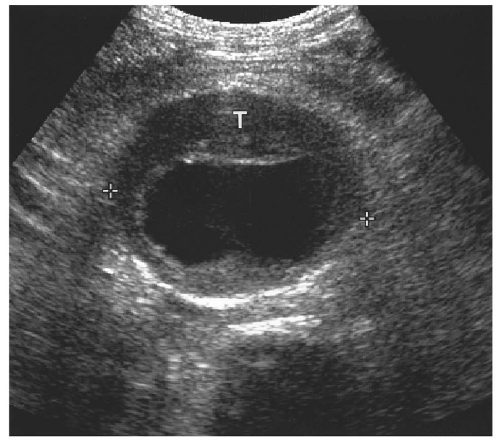 Figure 14.28. Abdominal aortic aneurysm (AAA). Transverse ultrasound image shows 6.8 cm in diameter AAA (electronic cursors). Note the mural thrombus (T) surrounding the lumen. |
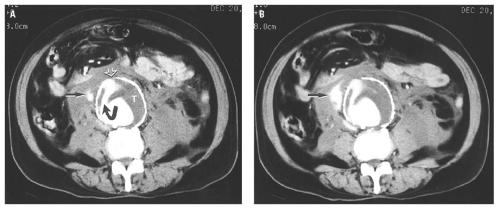 Figure 14.29. Ruptured abdominal aortic aneurysm. A: Enhanced CT image shows contrast material (curved arrow) leaking through mural thrombosis (T) and then through a gap (open arrow) in the calcified anterior wall of the aneurysm. Extravasated contrast material (arrow) is seen in the retroperitoneal hematoma on the right. B: Image at the same level made 3 minutes later shows an increased amount of extravasated contrast material (arrow). |
 Figure 14.30. Elderly man with severe left lower quadrant pain from the previous day. This large abdominal aortic aneurysm has a calcified wall. Note the highattenuation crescent inside the calcification (arrows), which indicates impending rupture. Abundant left retroperitoneal hematoma is further evidence of impending rupture. |
arterial extravasation when it is present (Fig. 14.33). An acute hematoma is hyperdense (70 to 90 HU). In hematomas that result from excessive anticoagulation, fluid cell levels and heterogeneity within the hematoma may be seen.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


