Simple fluid density (0-10 HU) or slightly hyperdense
Internal gas in absence of intervention/drainage highly suspicious for infected collection
“Abscess” suggests a discrete, drainable fluid collection: Differentiate from ill-defined inflammation and fluid that is not drainable (i.e. phlegmon)
Adjacent fat stranding, edema, and fascial thickening due to inflammation
Intraparenchymal abscess (liver, kidney, etc.) often surrounded by low-density parenchymal edema
• US: Complex fluid collection with internal low-level echoes, membranes, or septations
Increasing complexity within abscess fluid suggests thicker, more viscous contents
Greater complexity on US often implies greater difficulty in drainage (especially with small-caliber catheters)
Center of abscess avascular on color Doppler imaging, with peripheral hyperemia
PATHOLOGY
• Many different causes including postoperative setting, enteric perforation, generalized bacteremia, and trauma
CLINICAL ISSUES
• Increased incidence in diabetics, immunocompromised patients, and postoperative patients
DIAGNOSTIC CHECKLIST
• Differentiating abscess from noninfected collections after surgery may be difficult and requires correlation with clinical symptoms of infection or fluid aspiration
(Left) Axial CECT in an elderly postoperative patient demonstrates a rounded complex fluid collection with gas bubbles and an enhancing capsule , findings diagnostic for an abdominal abscess.
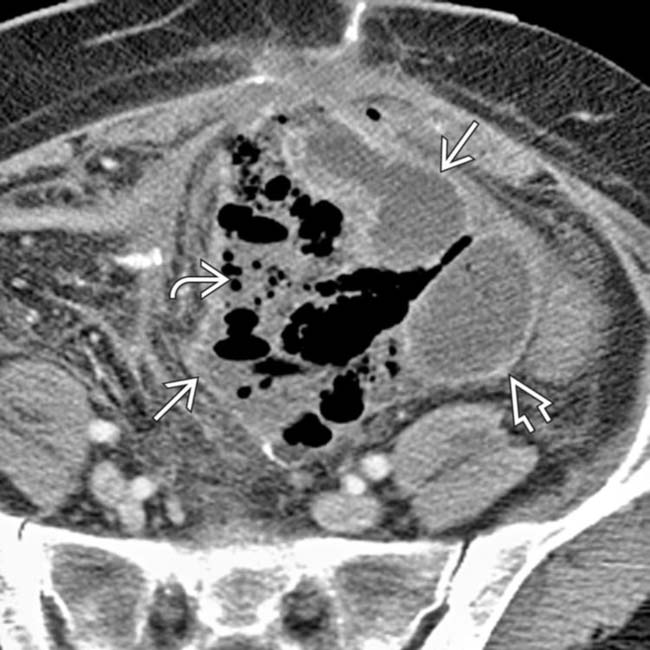
(Right) Axial CECT in a elderly postoperative patient demonstrates multiple loculated fluid collections with prominently enhancing capsules and mass effect on adjacent structures, representing abdominal abscesses. Note the air-fluid level within one of the abscesses.
(Left) Axial CECT shows a large pelvic abscess following hysterectomy. Note the presence of a discrete enhancing rim and mass effect on adjacent loops of bowel and the bladder.
(Right) Axial CECT shows placement of a percutaneous drainage catheter using a transgluteal approach. The abscess has almost completely resolved following drainage.
TERMINOLOGY
Definitions
• Localized abdominal collection of pus or infected fluid
IMAGING
General Features
• Best diagnostic clue
Loculated, encapsulated fluid collection with peripheral rim enhancement ± gas bubbles or air-fluid level on CECT
• Location
Can occur anywhere within abdominal cavity, including intraperitoneal space, extraperitoneal spaces, or intraparenchymal
• Size
Highly variable
– 2-15 cm in diameter, microabscesses < 2 cm
• Morphology
Low-density round or oval collection of fluid with a peripheral enhancing rim
CT Findings
• Low density, loculated, encapsulated fluid collection with peripheral rim enhancement
May be simple fluid density (0-10 HU) or slightly hyperdense
Often adjacent fat stranding, edema, and fascial thickening due to inflammation
• Presence of internal gas (∼ 50% of cases) in absence of intervention highly suspicious for infected collection
• Term “abscess” suggests a discrete, drainable fluid collection: Differentiate from ill-defined inflammation and fluid that is not drainable (i.e., phlegmon)
• Can be difficult to distinguish infected from noninfected (e.g., seroma, lymphocele, hematoma) collections
MR Findings
• Typically central core of abscess demonstrates fluid signal (low-signal T1WI, high-signal T2WI)
Internal complexity may slightly alter signal characteristics (e.g., hemorrhage, proteinaceous content)
• Enhancing peripheral rim on T1WI C+ images
• Abscesses anywhere in abdomen tend to show restricted diffusion (high signal on DWI with low ADC values)
Lower ADC values than noninfected fluid collections
– However, lack of restricted diffusion cannot exclude possibility of abscess (overlap in ADC values with necrotic tumors and noninfected collections)
• Usually evidence of adjacent soft tissue edema around abscess (high T2 signal)
Ultrasonographic Findings
• Complex fluid collection with internal low-level echoes, membranes, or septations on US
Dependent echoes represent debris within abscess
– Increasing complexity within abscess fluid suggests thicker, more viscous contents
– Greater complexity on US often implies more difficult drainage (especially with small-caliber catheter)
Posterior acoustic through transmission may vary depending on composition of fluid in abscess
– Abscesses with thick, viscous, proteinaceous fluid may have relatively little through transmission
Center of abscess is typically avascular on color Doppler imaging, with peripheral hyperemia
Fat surrounding abscess may appear markedly echogenic due to inflammation
– Inflamed fat hyperemic on color Doppler
Internal echogenic foci with ring-down artifact and posterior “dirty” acoustic shadowing suggest presence of gas
Radiographic Findings
• Radiography
Soft tissue “mass” or density ± internal ectopic gas (about 50% of cases) or air-fluid levels
– May be associated with loss of soft tissue-fat interface
Dilated bowel loops due to focal ileus
Subphrenic abscess often results in adjacent pleural effusion and lower lobe atelectasis
Fluoroscopic Findings
• Abscess sinogram
Useful after percutaneous drainage to assess presence of residual abscess cavity
Defines catheter position and communication with abscess
Identifies fistulization of abscess with adjacent bowel, pancreas, or biliary tree
Nuclear Medicine Findings
• Ga-67 scan
Most often utilized for chronic infections and fever of unknown origin
Nonspecific, as Ga-97 may demonstrate uptake with tumors, such as lymphoma, as well as chronic granulomatous processes (i.e., sarcoidosis)
• In-111 or Tc-99m-labelled white blood cell (WBC) scan
Most often utilized for acute infections or inflammatory bowel disease
73-83% sensitivity
False-positives with bowel infarct or hematoma
• Newer agents
Indium-labeled polyclonal IgG
Only gold members can continue reading. Log In or Register to continue

 “Abscess” suggests a discrete, drainable fluid collection: Differentiate from ill-defined inflammation and fluid that is not drainable (i.e. phlegmon)
“Abscess” suggests a discrete, drainable fluid collection: Differentiate from ill-defined inflammation and fluid that is not drainable (i.e. phlegmon)

 Greater complexity on US often implies greater difficulty in drainage (especially with small-caliber catheters)
Greater complexity on US often implies greater difficulty in drainage (especially with small-caliber catheters)

 with gas bubbles
with gas bubbles  and an enhancing capsule
and an enhancing capsule  , findings diagnostic for an abdominal abscess.
, findings diagnostic for an abdominal abscess.
 with prominently enhancing capsules
with prominently enhancing capsules  and mass effect on adjacent structures, representing abdominal abscesses. Note the air-fluid level
and mass effect on adjacent structures, representing abdominal abscesses. Note the air-fluid level  within one of the abscesses.
within one of the abscesses.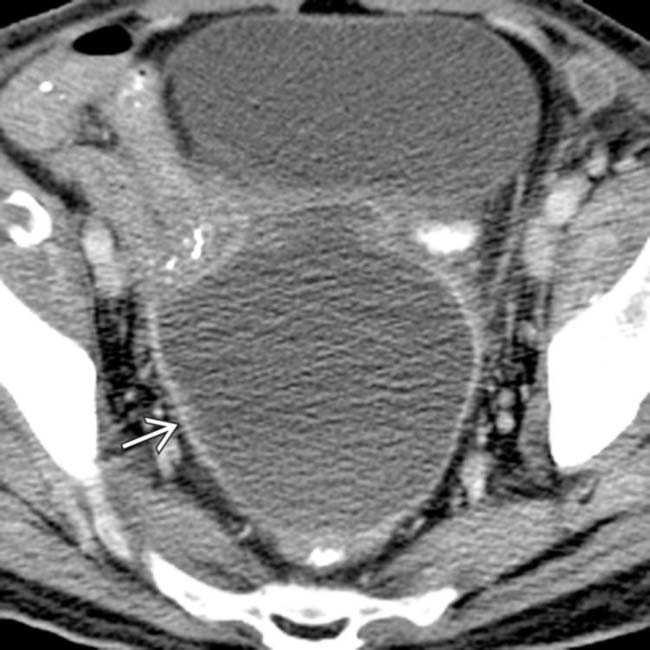
 following hysterectomy. Note the presence of a discrete enhancing rim and mass effect on adjacent loops of bowel and the bladder.
following hysterectomy. Note the presence of a discrete enhancing rim and mass effect on adjacent loops of bowel and the bladder.
 using a transgluteal approach. The abscess has almost completely resolved following drainage.
using a transgluteal approach. The abscess has almost completely resolved following drainage.































