Fig. 12.1
Transducer suitable for abdominal examination. 1–5 MHz phased array transducer; note the orientation marker
Machine Setup
Orientation
The orientation marker on the probe should be directed toward the patient’s head (cephalad: sagittal or coronal section; Fig. 12.2), but sometimes you may want to put the marker to the patient’s right to scan the body horizontally (transverse section; Fig. 12.3). On the screen, an orientation marker should be on the left upper corner of the screen.
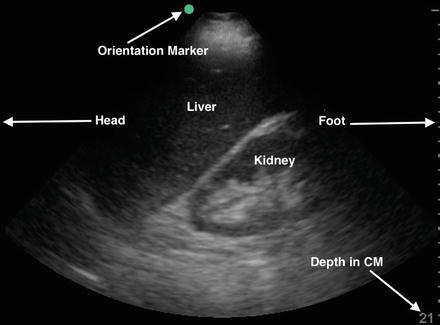
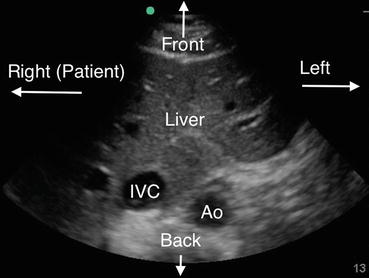
Fig. 12.2
Sagittal view of the right upper quadrant. The transducer is oriented with the probe marker toward the patient’s head (cephalad), corresponding to the left side of the screen (green-blue orientation dot). Also pay attention to the depth, which is 21 cm in this image
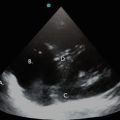
Fig. 12.3
Transverse view of the right upper quadrant. This time, the orientation marker on the transducer is facing patient’s right. This image is analogous to a transverse image on a CT scan of the abdomen. IVC inferior vena cava, Ao aorta. Note depth is 13 cm in this image
Depth
Start with the depth set at 13–19 cm, and, occasionally, even more depth is required. Always start with sufficient depth so that important structures or pathology located deep in the abdomen are not missed.
Gain
Overgain is another common error made by the novice ultrasonographer. Try to undergain as much as possible.
Figure 12.4 illustrates control layout on a typical portable ultrasound machine.
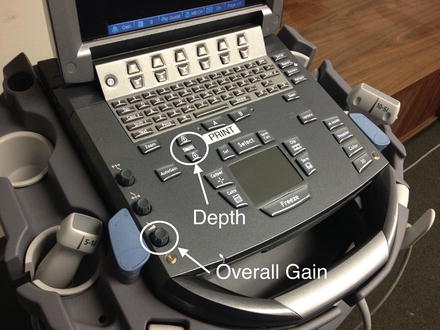
Fig. 12.4
Depth and gain controls. Though there are so many buttons on a console as shown above, important ones are very few (pictured: SonoSite M-Turbo, SonoSite Inc., Bothell, Washington, USA). Note each console (key layout) varies between machines
Patient Considerations for Abdominal Ultrasound in the ICU
The nature of the ICU patient may present several challenges to obtaining quality ultrasound images. Oftentimes, many of these obstacles can be overcome by technical or operator adaptations, and examples of such strategies are presented below.
The Obese Patient
If abdominal subcutaneous tissue is preventing an effective examination of the anterior abdomen, depth may be increased. If the machine function allows selection of different frequencies, choose a lower frequency for better penetration. Some structures, such as the inferior vena cava (IVC) or aorta, occasionally are better observed from a lateral approach.
Abdominal Gas
Gas has a high attenuation coefficient, meaning abdominal gas will prevent ultrasound from penetrating deep to a gas-filled viscus to examine other intra-abdominal structures. Performing ultrasound from a frontal approach is difficult in patients with abdominal gas. In such a setting, important vascular structures, such as the IVC and aorta, may not be well examined from a frontal examination, and laterally placing the probe in the anterior to mid-axillary line can prove helpful.
Supine Patients
Very few people in the ICU are not supine. The diaphragm may therefore be higher than expected in these patients. Therefore, identifying the diaphragm is of particular importance when you are planning procedures, such as thoracentesis or paracentesis. Scan higher in the thorax to definitively identify the diaphragm level prior to deciding on a spot for a procedure.
When examining the retroperitoneal organs, particularly the kidneys (especially the left one), a supine position makes the ultrasound more difficult. Place the transducer deep into the small space between the patient’s back and the bed. Sometimes help from other members of the critical care team in lifting the subcutaneous tissue or repositioning the patient is needed so that a space to scan can be created.
Other Patient Considerations: Age, Gender, and Body Size
Age, gender, and body size have to be taken into consideration as the size of organs is affected by the patient’s age, gender, or height. For example, longitudinal length of the kidney is longer in men and in younger or taller patients [1].
Competencies in Critical Care Abdominal Ultrasound
No definitive qualification or certification currently exists to dictate full competency in abdominal ultrasonography in the critically ill. In order to begin to help guide training programs and practicing critical care physicians, the American College of Chest Physicians (ACCP) and La Societe de Reanimation de Langue Française (SRLF) together published a statement on competence in critical care ultrasonography in 2009 [2].
Image Acquisition and Interpretation: A Location-Specific Approach to Abdominal Ultrasound in the ICU
Points of Interests: FAST Examination and the Location-Specific Approach
When imaging the abdomen, an ultrasonographer can take an organ-specific or a location-specific approach. A so-called organ-specific approach will focus on one specific organ at a time and then move, if desired, to the next organ. This is the typical approach taken in comprehensive abdominal ultrasounds performed in the radiology suite. Focused Assessment with Sonography for Trauma (FAST) examination [3] (see Chap. 14) is an example of a context-driven, location-specific ultrasound approach that was introduced to assess rapidly for the presence of free fluid as a sign of intraperitoneal injury following trauma. In the FAST exam, the examination is limited to a few key points of interest to allow a quick, stereotyped examination that can be carried out in the chaotic trauma bay. The concept of limiting the number of points of interest can be applied to the general critical care abdominal ultrasound as well.
A location-specific approach focuses on one specific point of examination, and all of the important organs are visualized from that location. This approach is efficient, and provides a logical and consistent framework to follow, so that with repeated examinations the ultrasonographer will gain confidence and experience in obtaining and interpreting a few critical views. There are inherent limitations in the comprehensiveness of this approach, and this must be kept in mind when assessing for specific pathologies, such as possible abdominal aortic aneurysm, in which imaging of a more complete extent of the organ is needed.
Point A: Right Upper Quadrant
Right mid- to anterior axillary line at the 8–10th intercostal space. What can be evaluated: right hemidiaphragm, liver, pleural effusion, ascites, right kidney, IVC, and aorta.
Point B: Subcostal Point
Common structures to be evaluated: IVC, aorta, pancreas, liver, gallbladder, common bile duct, ascites, and stomach.
Point C: Left Upper Quadrant
Left mid-axillary line at the 8–10th intercostal space.
Common structures to be evaluated: left hemidiaphragm, spleen, left kidney, and ascites.
Point D: Suprapubic Window
Structures to be evaluated: bladder, prostate gland, uterus, and ascites.
Point A: Right Upper Quadrant
Point A should be the starting point of an abdominal ultrasound examination in the critically ill. Not only can the diaphragm, liver, and right kidney be examined, but the IVC and aorta can also be imaged from this view. Below, I will describe each organ accessible from this viewpoint.
Right Hemidiaphragm
Examination of the diaphragm is important for two reasons [1]. The diaphragm is an important landmark that separates the abdomen from the thorax [2]. Evaluation of the diaphragm itself gives you important information in the critically ill. By observation of how much it thickens during inspiration, inspiratory muscle function can be assessed. Evaluation of diaphragmatic function is discussed in detail in Chap. 10.
Locating the diaphragm is of primary importance since this is the major structure that separates the abdomen from the thorax (Fig. 12.5). Since free fluid may be located above or below the diaphragm, failure to identify this structure may lead to preventable errors during procedures, such as an inadvertent sub-diaphragmatic puncture during a thoracentesis.
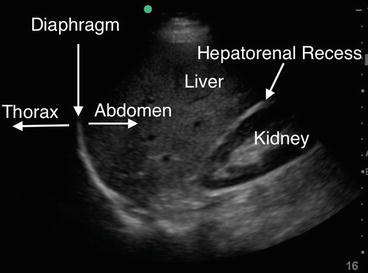
Fig. 12.5
Ultrasound image: right diaphragm, liver, and kidney. The diaphragm in this ultrasound image is the hyperechoic curved line. Do not confuse the diaphragm with the hyperechoic line in the hepatorenal recess (Morison’s pouch)
Technical Aspects: How to Locate the Diaphragm
When using the phased array 1–5 MHz transducer at Point A, the orientation marker should be facing cephalad (Fig. 12.6) or directed toward the right shoulder, thus slightly rotated to the back (parallel to rib). Place the transducer at the mid-axillary line at the level of the 8th to 10th intercostal space. The probe may be rotated so that the acoustic shadow of the rib does not interfere with the image.

Fig. 12.6
Position of the transducer at Point A. Start scanning at this point in a critical care abdominal ultrasound examination. Place the transducer in the right anterior to midaxillary line at the 8th–10th intercostal space to examine the right hemidiaphragm. Note the orientation marker is facing up (cephalad). The liver and kidney can be imaged here, as well as the diaphragm. Rotate the transducer (orientation marker) to 10–11 o’clock to minimize artifact from the rib cage (acoustic shadowing). Carefully select the depth (usually 16–19 cm) so that you do not miss important structures
Pitfalls and Precautions
Do not confuse the right hemidiaphragm with the hyperechoic line between liver and kidney representing Gerota’s fascia.
Supine patients usually have their diaphragm in higher position. Where you normally expect lung, there may be liver or kidney. Move the transducer cephalad and caudad freely to make sure you identify the diaphragm. If you have trouble finding the diaphragm, usually there are a few specific reasons:
1.
The transducer is positioned either too high (imaging the lung) or too low (imaging part of the liver or kidney).
2.
The transducer is placed too far anteriorly.
3.
The transducer rotation is suboptimal.
Right Kidney
With rare exception, every patient who comes to the ICU with acute renal failure or low urine output should have ultrasound scanning of the genitourinary system rapidly carried out to rule out obstruction (hydronephrosis, full bladder with outlet obstruction, etc.) and to assess for evidence of chronic kidney disease. When a UTI is suspected, look for fluid collections around the kidney and/or signs of hydronephrosis. Pathology can subsequently be confirmed with a comprehensive ultrasound, but early identification of these findings can allow appropriate early interventions, further imaging, and consultations to be initiated quickly.
Technical Aspects: Imaging the Right Kidney
To scan the kidney, start the scan from the mid- to posterior axillary line, moving slowly forward to the anterior axillary line. Start scanning from the back so that the hand holding the transducer is almost touching the bed when the patient is in a supine position. If orientation is lost, look for the diaphragm, an important landmark. Placing the patient in the left lateral decubitus position, if possible, may be helpful. The transducer may be rotated slightly to minimize the effect of the acoustic artifact from the rib cage. Novice examiners may find it difficult to locate the kidney; this is often due to the fact that they start scanning too far anteriorly. Because the kidney is a retroperitoneal organ, scanning from back to front allows the sonographer to identify the kidney more easily (this is particularly the case with the left kidney). Angulation is also important: angle the transducer so that the beam is aimed posteriorly, almost scanning in a sagittal plane, i.e., not with the beam in a perpendicular position (coronal view), which is more suitable for assessment of IVC and aorta. Look for free fluid in the hepatorenal recess (Fig. 12.7) between the right kidney and the liver (Morison’s pouch). Be sure to image the kidney through its inferior pole to avoid inadvertently missing free fluid in the most inferior aspect of Morison’s pouch.
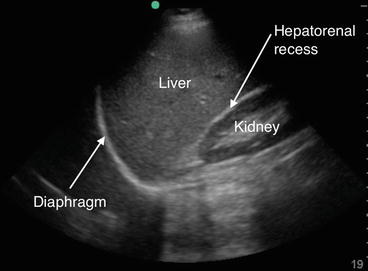
Fig. 12.7
The hepatorenal recess (Morison’s pouch). The potential space that exists between the kidney and the liver constitutes the hepatorenal recess, or Morison’s pouch. The echogenic line of Gerota’s fascia should not be confused with the echogenic pleural line of the diaphragm. Fluid accumulation in the hepatorenal recess will result in a relatively hypoechoic space forming between the liver and the kidney (see also Fig. 12.11 below)
Basic Competencies: Kidney
Goals when scanning the kidney include an assessment of kidney size, observation of the pelvis for evidence of hydronephrosis, and qualitative examination of renal cortex echogenicity. First, assess kidney size. Freezing an image and using calipers may be helpful. The size of the normal kidney usually ranges from 9 to 12 cm [1]. Reduction in kidney size typically indicates chronic/irreversible renal pathology, i.e., chronic kidney disease with atrophy [4]. Next, observe the renal pelvis to see if there is any sign of hydronephrosis (dilation of renal pelvis and collecting system) (Fig. 12.8). This will appear as hypoechoic regions that communicate and coalesce in the renal pelvis and drain into the ureter. More subtle evidence of early hydronephrosis may require comprehensive abdominal ultrasound for confirmation. Finally, assess the renal cortex. The normal renal cortex appears thick; a thin cortex suggests the presence of chronic kidney disease. In acute kidney injury, the cortex is usually hyperechoic. By contrast, in chronic kidney disease the renal cortex is usually thin and hypoechoic.
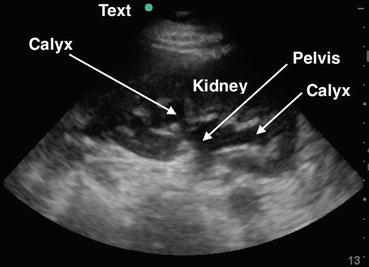
Fig. 12.8




Hydronephrosis: Note hypoechoic lesions which are dilated calyces connected to the renal pelvis. Unlike renal cysts, these structures can be shown to be connected. Move the transducer carefully to observe and document connectivity and drainage into the renal pelvis
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
