Findings identical to calculous cholecystitis (except gallstones)
Thickening of gallbladder wall > 3 mm
Positive sonographic Murphy sign
– May be absent or impossible to elicit in critically ill patients at highest risk
Gallbladder distention (> 5 cm in transverse plane)
Gallbladder wall hyperemia on color Doppler
• CT and MR
Gallbladder wall thickening (> 3 mm) with mural/mucosal hyperenhancement
– May be associated with intramural lucency on CT caused by wall edema (subserosal halo sign)
Dilated gallbladder (> 5 cm) with pericholecystic fluid and fat stranding
Hyperenhancement of liver adjacent to gallbladder
• Hepatobiliary scintigraphy
Nonvisualization of gallbladder 4 hours after injection of radiotracer (or 30 minutes after morphine)
TOP DIFFERENTIAL DIAGNOSES
• Acute calculous cholecystitis
• Gallbladder wall edema
• Hyperplastic cholecystoses
• Gallbladder carcinoma
• AIDS cholangiopathy
PATHOLOGY
• Not associated with obstruction of cystic duct by stones
• Most often result of bile stasis and gallbladder ischemia
• Typically occurs in critically ill patients (trauma, surgery, sepsis, mechanical ventilation, immunosuppression, etc.)
CLINICAL ISSUES
• Higher risk of morbidity/mortality compared to calculous cholecystitis with ↑ risk of complications
More likely than calculous cholecystitis to present atypically
Insidious presentation in critically ill patients and diagnosis is often delayed
• Preferred treatment: Cholecystectomy and broad spectrum intravenous antibiotics
• Cholecystostomy used as bridge to definitive cholecystectomy in critically ill, unstable patients
(Left) Coronal CECT in a critically ill ICU patient demonstrates severe gallbladder (GB) wall thickening and edema with pericholecystic fat stranding and fluid. Note the lack of clear enhancement of the GB wall near the fundus , concerning for gangrenous cholecystitis.
(Right) Coronal CECT acquired a day later shows placement of a cholecystostomy tube , a common temporizing measure in critically ill patients too unstable for cholecystectomy.
(Left) CECT of a diabetic septic female 4 days post laparotomy for a perforated duodenal ulcer shows a distended GB, wall thickening , and pericholecystic fat infiltration . No gallstones were identified at ultrasound.
(Right) Hepatobiliary scan of the same patient shows progressive small bowel filling but no GB activity 30 minutes post tracer administration. No GB activity was shown after morphine administration (an observation that increases exam specificity).
TERMINOLOGY
Definitions
• Acute inflammation of gallbladder (GB) unrelated to gallstones
IMAGING
General Features
• Best diagnostic clue
Combination of imaging features and clinical history
– Ultrasound: Distended GB with wall thickening, pericholecystic fluid, and positive sonographic Murphy sign but no gallstones
– Hepatobiliary scintigraphy: Nonvisualization of GB
• Findings identical to acute calculous cholecystitis (except for absence of gallstones)
Ultrasound often equivocal due to inability to elicit sonographic Murphy sign in intubated/unconscious patients
• Thickening of GB wall > 3 mm
Higher thresholds increase specificity, but decrease sensitivity
– Using cutoff value of 3 mm leads to better sensitivity but lower specificity
– Using cutoff value of 4 mm (or 5 mm) leads to better specificity at the cost of having more false-negative cases
Striated appearance of wall is common (no longer thought to be suggestive of gangrenous cholecystitis)
• Positive sonographic Murphy sign (pain with insonation over GB that is accentuated with deep breathing)
May be absent or impossible to elicit in critically ill ICU patients at highest risk for acalculous acute cholecystitis
• GB distention (> 5 cm in transverse plane)
• Pericholecystic echogenic fat (due to inflammation)
• GB wall hyperemia on color Doppler images
• Complications
Gangrenous cholecystitis: Asymmetric wall thickening, intraluminal linear membranes, and echogenic material due to sloughed mucosa and irregularity/ulcerations of GB wall
– May not be associated with wall hyperemia due to necrosis
Emphysematous cholecystitis: Intramural and intraluminal gas with multiple bright echogenic reflectors and “dirty” posterior acoustic shadowing
– Champagne sign: Tiny, nonshadowing echogenic foci rising up in real-time from dependent portion of GB
Perforated GB: Collapsed GB with discrete wall defect and adjacent pericholecystic fluid collection ± complex fluid in peritoneal cavity
– Most common site of perforation is fundus, which can be difficult to visualize in some patients
– Sonographic hole sign: Visualization of defect in GB wall is more easily diagnosed on CT
Hemorrhagic cholecystitis: Echogenic clot within GB
CT Findings
• Imaging findings are identical to acute calculous cholecystitis (except for absence of gallstones)
• Uncomplicated acalculous cholecystitis
GB wall thickening (> 3 mm) with mural and mucosal hyperenhancement
– May be associated with intramural lucency caused by wall edema (subserosal halo sign)
Pericholecystic fluid and fat stranding
Hyperenhancement of liver adjacent to GB (most apparent in arterial phase)
Dilated GB (> 5 cm in diameter)
• Complicated acalculous cholecystitis
Gangrenous cholecystitis: Hypoenhancement or nonenhancement of portions of GB wall
– May be associated with small sites of ulceration or outpouchings in GB wall
– Often associated with asymmetric wall thickening
– Intraluminal linear strands due to sloughed mucosa
Emphysematous cholecystitis: Intramural or intraluminal gas with other findings of cholecystitis
Hemorrhagic cholecystitis: High-density blood within GB ± blood in intrahepatic/extrahepatic ducts
– May be associated with active extravasation (usually best visualized on arterial phase)
Only gold members can continue reading. Log In or Register to continue










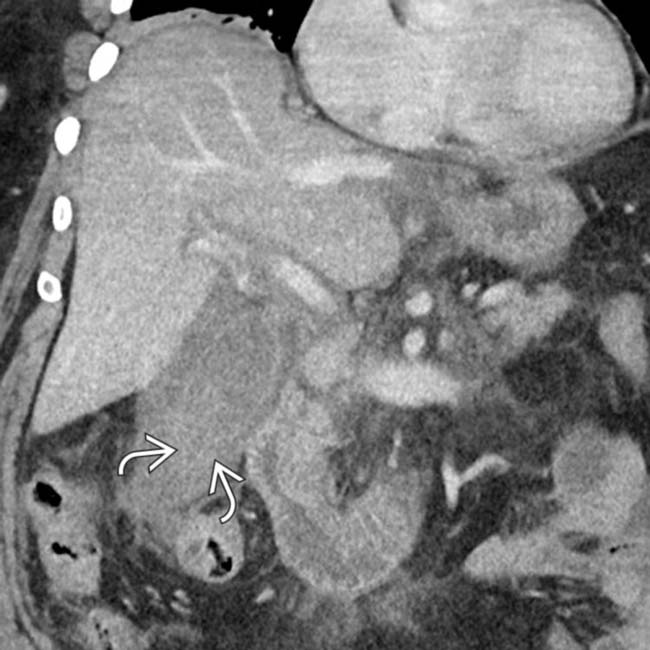
 , concerning for gangrenous cholecystitis.
, concerning for gangrenous cholecystitis.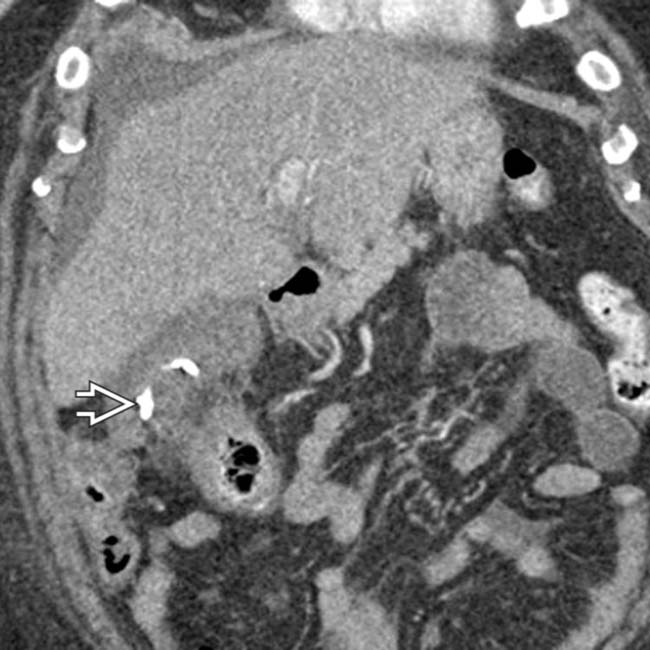
 , a common temporizing measure in critically ill patients too unstable for cholecystectomy.
, a common temporizing measure in critically ill patients too unstable for cholecystectomy.
 , and pericholecystic fat infiltration
, and pericholecystic fat infiltration  . No gallstones were identified at ultrasound.
. No gallstones were identified at ultrasound.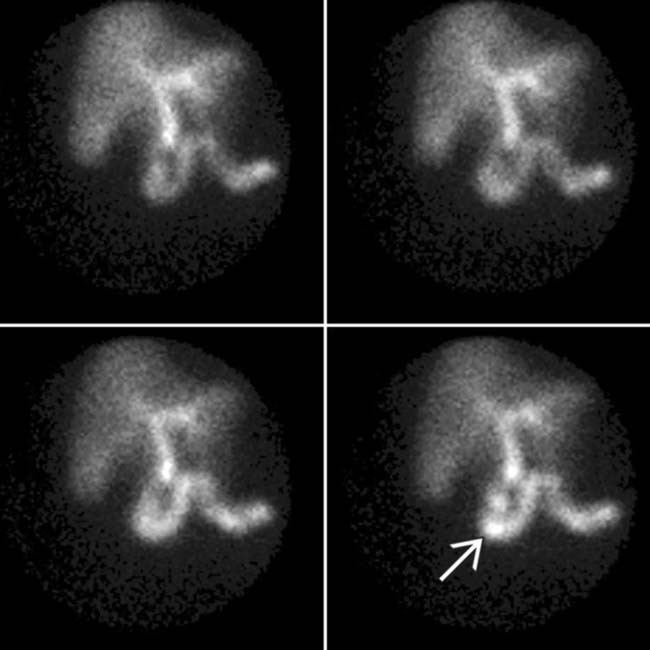
 but no GB activity 30 minutes post tracer administration. No GB activity was shown after morphine administration (an observation that increases exam specificity).
but no GB activity 30 minutes post tracer administration. No GB activity was shown after morphine administration (an observation that increases exam specificity).




 Gangrenous cholecystitis: Asymmetric wall thickening, intraluminal linear membranes, and echogenic material due to sloughed mucosa and irregularity/ulcerations of GB wall
Gangrenous cholecystitis: Asymmetric wall thickening, intraluminal linear membranes, and echogenic material due to sloughed mucosa and irregularity/ulcerations of GB wall Emphysematous cholecystitis: Intramural and intraluminal gas with multiple bright echogenic reflectors and “dirty” posterior acoustic shadowing
Emphysematous cholecystitis: Intramural and intraluminal gas with multiple bright echogenic reflectors and “dirty” posterior acoustic shadowing Perforated GB: Collapsed GB with discrete wall defect and adjacent pericholecystic fluid collection ± complex fluid in peritoneal cavity
Perforated GB: Collapsed GB with discrete wall defect and adjacent pericholecystic fluid collection ± complex fluid in peritoneal cavity




 Hemorrhagic cholecystitis: High-density blood within GB ± blood in intrahepatic/extrahepatic ducts
Hemorrhagic cholecystitis: High-density blood within GB ± blood in intrahepatic/extrahepatic ducts







