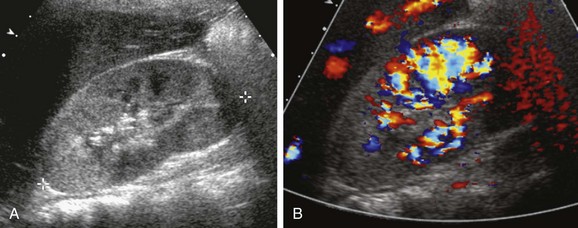
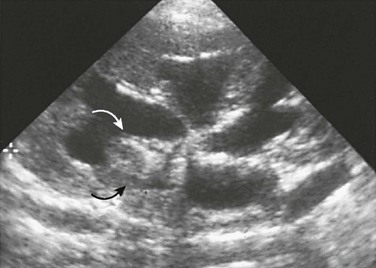
Chapter 115 Acute Bacterial Pyelonephritis Overview: The term pyelonephritis encompasses infections of the renal parenchyma and pelvocaliceal system. Bacterial infections of the kidneys are further categorized as acute or chronic, unilateral or bilateral, and focal, multifocal, or diffuse. Potential complications of pyelonephritis include renal or perinephric abscess. A bacterial infection in which purulent material fills a dilated collecting system is termed pyonephrosis.1 Pathophysiology and Clinical Presentation: The most common cause of acute bacterial pyelonephritis is ascending infection from the lower urinary tract. Parenchymal renal infection occasionally occurs as a result of hematogenous inoculation; this mechanism is more common in infants than in older children. Although children with vesicoureteral reflux are at elevated risk for pyelonephritis, reflux is not a prerequisite for renal infection. Potential clinical manifestations of acute bacterial pyelonephritis include flank pain, abdominal pain, fever, pyuria, nausea, and vomiting. Young infants with pyelonephritis often have nonspecific findings such as irritability and poor feeding; fever is sometimes lacking.2–4 Imaging: Renal cortical scintigraphy with technetium-99m dimercaptosuccinic acid (DMSA) or technetium-99m glucoheptonate is highly sensitive (at least 90%) for the detection of acute bacterial pyelonephritis. Infected regions of the kidneys have diminished or absent accumulation of the radiopharmaceutical agent, often with a spherical or flarelike pattern (Fig. 115-1). A renal abscess produces a scintigraphic defect that usually is indistinguishable from that of uncomplicated parenchymal infection.5,6 Figure 115-1 Acute bacterial pyelonephritis. Contrast-enhanced computed tomography (CT) provides sensitivity that is similar to renal cortical scintigraphy for the diagnosis of acute bacterial pyelonephritis. Infected renal parenchyma has diminished contrast enhancement on images obtained immediately after injection of contrast material (Fig. 115-2). Potential patterns of infected parenchyma include radially oriented linear streaks of diminished attenuation, round or irregular hypoattenuating foci, wedge-shaped defects, and heterogeneous diminished enhancement throughout an enlarged kidney. The nephrogram intensity usually is diminished relative to the contralateral normal kidney. Delayed CT images of the infected kidney show retention of contrast in obstructed tubules. A parenchymal abscess appears as a hypoattenuating focus, sometimes with a prominently enhancing rim. A perinephric abscess also is hypoattenuating.7 Figure 115-2 Multifocal bacterial pyelonephritis. Renal parenchymal edema resulting from infection leads to diminished signal intensity on T1-weighted magnetic resonance imaging (MRI) and increased signal intensity on T2-weighted images (Fig. 115-3). Nephromegaly or localized parenchymal expansion may be present. Corticomedullary differentiation is sometimes deficient. The parenchyma may have a striated appearance. Edema in the perinephric space is a common MRI finding. As with CT, contrast enhancement is deficient in the involved portions of parenchyma. Urothelial thickening is sometimes appreciable.8,9 Figure 115-3 Acute bacterial pyelonephritis. Reported sensitivities of sonography for the detection of acute bacterial pyelonephritis range from 25% to 50%. The findings include nephromegaly, abnormal parenchymal echogenicity, loss of corticomedullary differentiation, renal sinus hyperechogenicity, and urothelial thickening. Color Doppler or power Doppler imaging demonstrates diminished perfusion of the infected regions of parenchyma, sometimes with a wedge shape (Fig. 115-4). A parenchymal abscess usually appears as a spherical hypoechoic focus with acoustic enhancement. Occasionally, pus within the cavity results in an isoechoic or hypoechoic appearance. A perinephric abscess appears as a hypoechoic fluid collection immediately peripheral to the capsule.10–13 Treatment and Follow-up: Longer and more intensive antibiotic therapy is required for upper urinary tract infections than for those confined to the bladder. Antibiotic prophylaxis against reinfection is indicated for selected patients, particularly for those with predisposing factors. The utility of follow-up diagnostic imaging studies for children with acute bacterial pyelonephritis is a topic of ongoing investigation and debate.14,15 Overview: Pyonephrosis is a bacterial infection of the kidney in which purulent material fills a dilated collecting system. Most often, a preexisting chronic obstruction is present, such as congenital ureteropelvic junction obstruction. Acute obstruction because of a calculus is an occasional cause in children. The clinical presentation of pyonephrosis is similar to that of other bacterial urinary tract infections. Fever, flank pain, pyuria, and hematuria are common.16 Imaging: Sonography shows echogenic material within a dilated pelvocaliceal system (Fig. 115-5). The purulent material often layers in the dependent portions of the collecting system and may shift with changes in patient position. Thickening of the wall of the dilated renal pelvis usually is present. Uncommon additional potential findings include a fluid-debris level in the collecting system, echogenic foci due to gas-forming organisms, and complete filling of the dilated collecting system with echogenic material.17,18 Figure 115-5 Pyonephrosis. Imaging of pyonephrosis with CT, MRI, or scintigraphy shows diminished function of the involved kidney. Deficient excretion of intravenously administered contrast or radiopharmaceutical material is noted. Contrast enhancement of the renal parenchyma of the infected kidney is heterogeneous and delayed on CT. Excreted contrast may outline filling defects in the dilated collecting system on delayed images. Debris usually is visible in the dilated renal collecting system on MRI. The renal parenchyma has abnormal heterogeneous signal intensity. The pus-filled collecting system is markedly hyperintense on diffusion-weighted images. Contrast-enhanced MRI confirms reduced function of the kidney.19 Treatment and Follow-up: The treatment of pyonephrosis includes prompt initiation of aggressive antimicrobial therapy. Drainage of the obstructed collecting system often is required, usually by percutaneous nephrostomy. Surgical correction of the underlying obstruction typically is performed after resolution of the acute infection. Overview: Xanthogranulomatous pyelonephritis (XGP) is an uncommon form of severe chronic renal parenchymal infection. The pathogenesis typically involves chronic infection of an obstructed kidney. Histologic examination demonstrates inflammatory cells interspersed within fibrogranulomatous tissue, nodules of lipid laden macrophages, and areas of necrotic parenchyma. Diffuse involvement of the kidney is most common; segmental or focal forms also can occur, sometimes in association with obstruction of a duplicated system or infundibulum. Common clinical findings include fever, flank pain, malaise, pyuria, weight loss, and anemia.20–22 Imaging: In the early stages of XGP, the involved portion of the kidney typically has an irregular hyperechoic character on sonography. With the diffuse form, the kidney may be massively enlarged but usually maintains a reniform shape. Echogenic foci with shadowing indicate the presence of calcifications. With progression, necrotic tissue and fluid are usually hypoechoic. Echogenic debris is sometimes visible within abscesses or the dilated collecting system.23 CT of diffuse XGP typically demonstrates an enlarged nonfunctioning kidney that has multiple low-attenuation parenchymal foci (Fig. 115-6). A staghorn calculus often is present in a contracted renal pelvis. Irregular contrast enhancement of the inflamed renal parenchyma occurs, often accompanied by inflammatory enhancement of the perinephric fat. Abscesses are moderately hypoattenuating and do not enhance with contrast. The pus-filled collecting system also is hypoattenuating. Little or no contrast excretion occurs. Regional retroperitoneal lymphadenopathy is common. With the focal form of XGP, CT typically demonstrates an expansile renal mass. Peripheral granulation tissue or compressed renal parenchyma may result in an enhancing peripheral rim. The involved renal parenchyma typically has low or intermediate signal intensity on T1-weighted MRI and high intensity on T2-weighted images.24 Figure 115-6 Xanthogranulomatous pyelonephritis. Treatment and Follow-up: The usual treatment for XGP is antibiotic therapy followed by nephrectomy or heminephrectomy. A percutaneous biopsy occasionally is useful to allow differentiation from a neoplasm and to provide material for culture. With acute disease, percutaneous abscess drainage can serve as a temporizing measure. Overview: Candidiasis, typically due to Candida albicans, accounts for about 80% of renal fungal infections. Premature neonates are particularly susceptible. The clinical presentation in neonates usually is nonspecific: hypertension, oliguria, or anuria. Older children with renal candidiasis usually have immunocompromise. The clinical findings typically are indistinguishable from those of a bacterial infection: fever, chills, dysuria, and flank pain.25 Imaging: Potential sonographic findings of renal candidiasis include parenchymal hyperechogenicity, nephromegaly, one or more small abscesses, and debris within the collecting system. A fungus ball (mycetoma) in the pelvocaliceal system appears as an echogenic object, with or without acoustic shadowing (Fig. 115-7). Dilation of the collecting system proximal to a fungus ball is common. Findings on contrast-enhanced CT include nephromegaly, diffuse or multifocal edema, renal abscess, and hydronephrosis. Infected parenchyma lacks normal contrast enhancement. Disseminated candidiasis sometimes results in tiny bilateral renal lesions, which often are associated with splenic and hepatic disease. CT may demonstrate organ enlargement and a heterogeneous (salt and pepper) pattern of contrast enhancement.26,27 Treatment and Follow-up: The typical treatment for renal candidiasis is systemic antifungal medication. Percutaneous nephrostomy is an option for children with an obstructing fungus ball. This treatment allows decompression of the collecting system and provides a pathway for installation of antifungal medication.
Acquired Abnormalities (Stone Disease and Infection)
Renal Infection
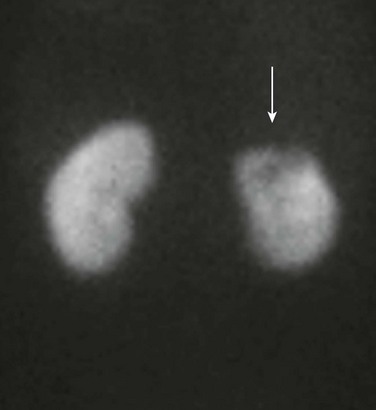
A posterior technetium-99m dimercaptosuccinic acid image of a febrile 16-year-old shows absent uptake in the upper pole of the left kidney (arrow).

Multiple areas of deficient contrast enhancement of the kidneys are present on this coronal computed tomography image of a 6-year-old girl.
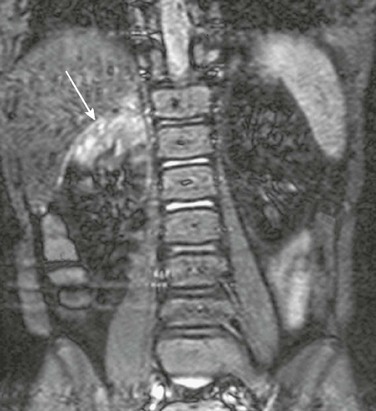
A coronal contrast-enhanced short tau inversion recovery magnetic resonance image shows abnormal increased signal in the upper pole of the right kidney (arrow). Normal renal parenchyma is hypointense. (Courtesy Damien Grattan-Smith, MD, Atlanta, GA.)
Pyonephrosis

A longitudinal sonogram shows a hydronephrotic duplex collecting system. Echogenic debris is present within the upper pole collecting system and ureter (arrows). Lesser debris is present within the lower pole collecting system.
Xanthogranulomatous Pyelonephritis

Contrast-enhanced computed tomography shows a right kidney that contains multiple stones surrounded by low-attenuation regions of abscess or necrosis. The process extends into the perirenal tissues, which are edematous and poorly defined, and into the soft tissues beneath the right abdominal wall, which are thickened. Metal-induced artifacts are produced by spinal fixation hardware in this child with dysraphism.
Candidiasis