Fig. 1
Relationship of prostate to surrounding anatomic landmarks on MRI T2-weighted sequences in a patient with clinically organ-confined disease. Left: Coronal view Right: Axial view
Four zones can be identified within the prostate of younger men (peripheral, central, transition, anterior fibromuscular). The peripheral zone lies adjacent to the rectum and is the site of the majority of tumors.
Local tumor spread by extracapsular extension (ECE) is facilitated by defects in the prostatic capsule at the sites of entry of neurovascular structures (suggesting the importance of perineural invasion) or glandular ducts and at the prostatic apex, where the capsule is thin or absent. While involvement of the bladder neck and even trigone is more easily identified on workup, care must be taken not to underestimate the potential for spread into and beyond the anterior fibrostroma, where transrectal ultrasound (TRUS) and biopsy may undersample. Spread to the rectum is rare due to the reinforcement of the Denonvilliers fascia, formed by invagination of a peritoneal layer between the two structures.
Regional spread is most common to the obturator lymph nodes and can also involve internal iliac, external iliac, and presacral nodes. Distant spread is overwhelmingly to bone, a predilection which is attributed to various hypotheses, including the anatomic ease of spread via the valveless Batson’s venous plexus to the lumbar spine and biologic rationale. In particular, this causes concern for pathologic fracture from involvement of long bones and the pelvis, spinal cord compression or spinal instability from vertebral involvement, and cranial nerve palsies from skull base involvement.
3 Diagnostic Workup Relevant for Target Volume Delineation
Initial case workup includes digital rectal examination, urinary and erectile function scores, and relevant labs. A history of prior transurethral resection of the prostate (TURP) or medication for benign prostatic hypertrophy is particularly important for optimizing treatment selection. In addition, knowledge of prior urethral surgery or visualization of the TURP defect is helpful so as to contour this area to insure that excessive doses are not given to this region.
Standard imaging includes TRUS for initial assessment of gland size and biopsy guidance, with tumors appearing hypoechoic. The TRUS volume is also helpful for it provides prognostic data such as PSA density. Computed tomography (CT) of the pelvis provides limited information regarding evaluation for pelvic adenopathy. While the literature on its sensitivity is mixed, suspicious nodes may be noted for biopsy when carrying the potential to affect treatment.
Magnetic resonance imaging (MRI) with 3T strength and with or without endorectal coil based on patient tolerance and level of detail needed (i.e. neurovascular bundle approximation relative to tumor prior to nerve sparing surgery is best seen with 3T + coil) is recommended at MSKCC for evaluation of intraprostatic anatomy and for ECE. This is performed at least 8 weeks following biopsy to allow for post-procedure changes to resolve. Tumors appear hypointense on T2 compared with normal gland, allowing assessment for dominant lesions and seminal vesicle invasion (Fig. 2). While blood products can also be hypointense on T2, they are hyperintense on T1, in contrast to tumor, allowing differentiation (Fig. 3). Disruption or irregularity of the well-defined capsule by tumor suggests ECE (Fig. 4). Sagittal view allows assessment of the extent of prior TURP defects and obstructive physiology, such as from a hypertrophied median lobe (Fig. 5). Finally, in the case of patients with MR-compatible prior hip arthroplasty, MRI fusion with CT-simulation images may facilitate basic visualization of target structures.
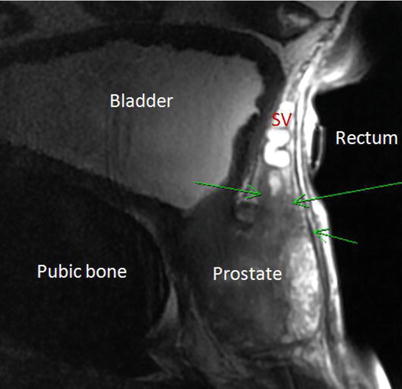
Fig. 2
Seminal vesicle (SV) invasion by tumor (green arrows) is demonstrated on sagittal MRI T2-weighted sequence by irregular hypointense signal encroaching upon the hyperintense proximal SV
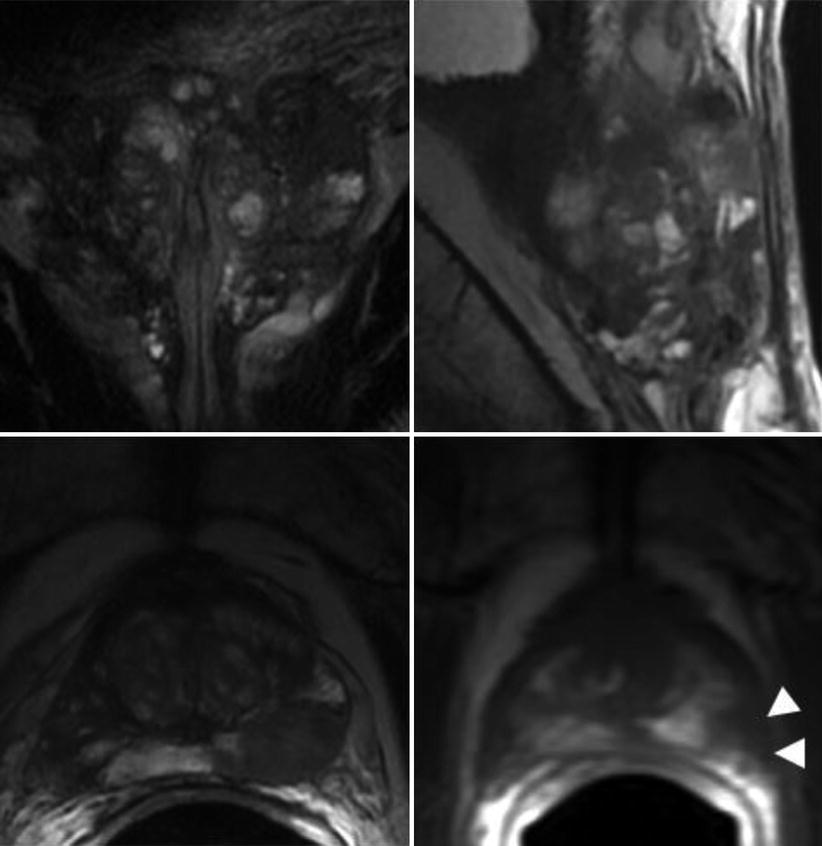
Fig. 3
Demonstration of post-biopsy changes on MRI, which limits interpretation of disease extent. Diffuse signal irregularities are noted on T2-weighted sequences in the coronal (top left), sagittal (top right), and axial planes (bottom left), as well as on T1-weighted sequence in the axial plane (bottom right). Nonetheless, the distinct hypointensity in the left posterolateral gland on both T1- and T2-weighted sequences suggests a dominant peripheral zone tumor (white arrowheads)
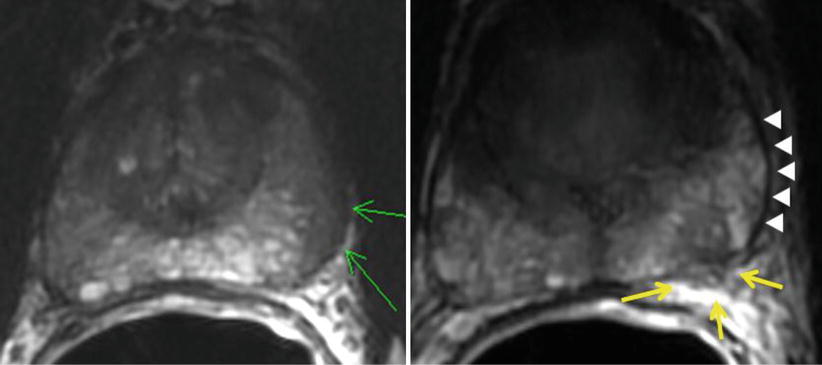
Fig. 4
Extracapsular extension (ECE) detected by MRI T2-weighted axial sequences of the prostate. Left: Broad capsular contact is shown (green arrows) along the left posterolateral boundary without frank disruption. This would be called suspicious but not definite for ECE. Right: In contrast, this image demonstrates a focal penetration (yellow arrows) of the capsule (white arrowheads) by a hypointense lesion, consistent with clear ECE
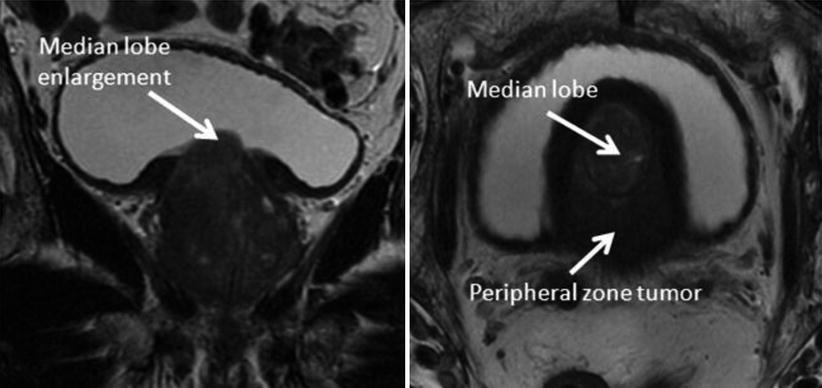
Fig. 5
MRI T2-weighted sequences (left coronal, right axial) demonstrate enlargement of the median lobe of the prostate with invagination into the bladder due to both tumor and hypertrophy. Such features can be mistaken for bladder neck thickening on CT slices alone, leading to inadequate tumor coverage by PTV. In this case, this invagination of tissue into the bladder should be treated
4 Simulation and Daily Localization
CT simulation is performed with 2–3 mm slice thickness. Our approach at MSKCC includes:
Get Clinical Tree app for offline access
Immobilization: Mold such as Aquaplast® in supine position with arms on chest and out of field.
Scan: Even if not treating pelvic nodes, scan cranial to prostate to allow full delineation of bladder, rectum to rectosigmoid junction, and the relevant areas of small bowel that may fall adjacent to high-dose distributions.
Image guidance: Gold fiducials or CalypsoTM beacons for daily inter-fraction or intra-fraction guidance, respectively, are placed at least 5 days prior to simulation.
Preparation: Bowel prep night prior, and oral contrast 90 min before simulation.
Special cases/regimens:
Full bladder – 2 cups of water 45 min before scan.
This is required in postoperative therapy due to the tendency of small bowel to fall into the prostatectomy bed. If this is not achieved, a cone down may be required.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree