E. Edmund Kim1, 2, Vanessa Murad3, 4, Jin-Chul Paeng5, Hyung-Jun Im6, Ji-Young Kim7 and Gi-Jeong Cheon5
(1)
Department of Radiological Sciences, University of California, Irvine, School of Medicine, Orange, CA, USA
(2)
Department of Nuclear Medicine and Department of Molecular Medicine, Graduate School of Convergence Science and Technology, Seoul National University College of Medicine, Seoul, Republic of Korea
(3)
Department of Nuclear Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea
(4)
Department of Diagnostic Imaging, Fundacion Santa Fe de Bogotá University Hospital, Bogota, Colombia
(5)
Department of Nuclear Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea
(6)
Departments of Applied Bioengineering, Molecular Medicine, and Biopharmaceutical Sciences, Graduate School of Convergence Science and Technology, Seoul National University, Seoul, Republic of Korea
(7)
Department of Nuclear Medicine, Bundang Seoul National University Hospital, Seoul Korea, Radiation Health Research Institute, Korea Hydro & Nuclear Power Co., Ltd., Seoul, Republic of Korea
Single-photon emission computed tomography (SPECT) imaging has evolved rapidly during the past decades since the introduction of the Anger camera in 1970, the posterior rotating gantry and dual detectors with better reconstruction processes, and quantitative data analysis. In the late 1990s, hybrid SPECT/CT imaging appeared to improve diagnostic accuracy with precise anatomical location and image quality with attenuation correction. In the last 10 years, the improvements in this equipment and the evolution in radiopharmaceuticals have allowed us to improve in the evaluation of physiological processes and in the characterization of pathologies based on morphological patterns [1]. Conventional analog technologies have advanced to multidetector devices with direct conversion digital detectors that improve efficiency, resolution and image quality, resulting in faster studies with lower doses and even the ability to image multiple radionuclides simultaneously. This includes the last generation cadmium-zinc-telluride (CZT) scanners, which bring more possibilities in research and clinical practice, especially in nuclear cardiology [2–4]. There is no denying that SPECT is still the go-to choice for most cardiologists.
There are multiple SPECT/CT applications, and in this chapter, we introduce most of them with demonstrative examples. In tumor pathology, its best-known applications are the evaluation of bone tumors, especially osteoblastic metastases, neuroendocrine tumors, and parathyroid adenomas [5, 6]. However, there are other multiple uses such as the evaluation of hepatocellular carcinoma, liver metastasis, neuroblastoma, paraganglioma, and thyroid cancer. In non-tumor bone pathology, it is indicated in trauma, degenerative disease, and infection, for example – also in the evaluation of benign thyroid pathology, gastrointestinal bleeding, lymphatic system pathology, and pulmonary physiology, among others [5, 7–9]. SPECT systems as well as radiopharmaceuticals are more available and probably cost-effective than PET, so they remain and will remain at the forefront.
1 Tumors
1.1 Hepatocellular Carcinoma
1.1.1 Case 1
A 51-year-old man with a diagnosis of hepatocellular carcinoma. Selected SPECT (top) and SPECT/CT (bottom) of the liver with 99mTc-MAA particles injected into a hepatic arterial catheter showed several focal areas of slightly to moderately increased activity in the right and left hepatic lobes corresponding to multicentric hepatoma. Only 50% of hepatomas can be imaged with FDG-PET, mainly because of the high levels of phosphatase that dephosphorylate FDG and allow it to diffuse out of cells (Fig. 1) [10].
Fig. 1
99mTc-MAA SPECT/CT
1.2 Liver Metastases
1.2.1 Case 1
A 68-year-old female patient with liver metastasis from breast cancer. Selected SPECT (top) and SPECT/CT (bottom) of the liver with 99mTc-MAA into the hepatic arterial catheter showed markedly heterogeneous activity in the liver caused by known metastases. There was no extra hepatic activity (Fig. 2) [11].
Fig. 2
99mTc-MAA SPECT/CT
1.2.2 Case 2
Selected SPECT (top) and SPECT/CT (bottom) of the upper abdomen with 99mTc-MAA particles into a hepatic arterial catheter showed curvilinear activity along the gastric wall, indicating the suboptimal position of the hepatic arterial catheter (Fig. 3) [12].
Fig. 3
99mTc-MAA SPECT/CT
1.2.3 Case 3
A 57-year-old female patient with hepatic metastasis of breast cancer. Selected SPECT (top) and SPECT/CT (bottom) images of the liver with 90Y microspheres injected into a hepatic arterial catheter showed increased activity in the right and left hepatic lobes, corresponding to metastatic lesions (Fig. 4) [13].
Fig. 4
90Y SPECT/CT
1.3 Neuroendocrine Tumors
1.3.1 Case 1
A 51-year-old male patient with chest tightness and dyspnea. He had prior history of a pancreatic neuroendocrine tumor, so 111In-octreotide SPECT/CT was done. Images showed focal increased activity in a soft tissue mass at the pericardium, which was posteriorly confirmed to be a metastatic lesion (Fig. 5) [14].
Fig. 5
1. Paraspinalis muscle
2. Transverse process
3. Vertebral body
4. Rib
5. Liver
6. Sternum
7. Left ventricle
8. Metastasis in pericardium
9. Left lower lobe of lung
10. Descending aorta
11. Left kidney
1.3.2 Case 2
A 72-year-old male patient with a history of midgut carcinoid. He attended with right shoulder and abdominal pain. 111In-octreotide SPECT/CT was performed, finding focal increased activity in the right glenoid at a slerotic lesion and the right hepatic lobe at a large necrotic mass. Posterior biopsy confirmed the diagnosis of metastatic neuroendocrine tumor (Fig. 6) [15].
Fig. 6
1. Right subscapularis muscle
2. Metastasis in right scapula neck
3. Right supraspinatus muscle
4. Right humerus
5. Right clavicle
6. Left pectoralis minor muscle
7. Left pectoralis major muscle
8. Vertebral body
9. Liver metastasis with central necrosis
1.3.3 Case 3
A 71-year-old male patient with abdominal pain, diarrhea, and elevated chromogranin A. 111In-octreotide SPECT/CT was performed, finding marked increased activity in a large pancreatic tail mass, as well as diffuse, increased activity in the portal vein. Surgical resection confirmed the diagnosis of a pancreatic neuroendocrine tumor with portal vein invasion (Fig. 7) [16].
Fig. 7
1. Neuroendocrine tumor in the pancreatic tail
2. Abdominal aorta
3. Vertebral body
4. Neuroendocrine tumor in the portal vein
5. Liver, S6
6. Liver, S5
7. Liver, S4
8. Liver, S1
9. Stomach
10. Spleen
1.3.4 Case 4
A 62-year-old female patient with a history of midgut carcinoid. She presented with cough, dyspnea, and abdominal pain, so 111In-octreotide SPECT/CT was done. Images showed a large mass in the right adrenal gland without abnormal increased activity. Also, diffuse, increased activity was noted in a consolidation at the right upper lung. Posterior biopsy of both lesions confirmed a right adrenal carcinoma and a metastatic neuroendocrine tumor in the right upper lung (Fig. 8) [17].
Fig. 8
1. Aortic arch
2. Vertebral body
3. Neuroendocrine tumor in RUL
4. Trachea
5. Right adrenal cancer
1.3.5 Case 5
A 54-year-old female patient with a history of rectal carcinoid. She developed abdominal pain and elevated serum levels of chromogranin A were found. 111In-octreotide SPECT/CT was performed, finding multifocal increased uptake in the right hepatic lobe at several biopsy confirmed metastasis (Fig. 9) [18].
Fig. 9
1. Left kidney
2. Vertebral body
3. Right kidney
4. NE tumor in liver S6
5. NE tumor in liver S5
6. Abdominal aorta
1.3.6 Case 6
A 74-year-old female patient with abdominal pain and diarrhea. 111In-octreotide SPECT/CT was done, finding focal increased activity in the pancreatic head. The surgical diagnosis was a pancreatic neuroendocrine tumor (Fig. 10) [21].
Fig. 10
1. Spleen
2. Abdominal aorta
3. Liver
4. Gallbladder
5. NE tumor in pancreatic body
6. Stomach
1.3.7 Case 7
A 67-year-old male patient with hypertension, abdominal pain, and palpitations. Elevated urinary catecholamines were found, so 123I-MIBG SPECT/CT was performed. Images showed focal increased uptake in a left adrenal mass which was confirmed as a pheochromocytoma (Fig. 11) [22].
Fig. 11
1. Spleen
2. Abdominal aorta
3. Liver, S6
4. Liver, S5
5. IVC
6. Portal vein
7. Stomach
8. Left adrenal pheochromocytoma
1.3.8 Case 8
A 68-year-old female patient with a history of midgut carcinoid developed chest pain and dyspnea. Chest X-ray showed a newly developed lung nodulex nodule and she had elevated serum levels of chromogranin A, so 111In-octreotide SPECT/CT was done. Images showed focal increased uptake in the right upper lung nodule, which was confirmed to be a metastatic neuroendocrine tumor (Fig. 12) [25].
Fig. 12
1. Left main bronchus
2. Right main bronchus
3. Rib
4. Neuroendocrine tumor metastasis in right lung
5. Ascending aorta
6. Pulmonary trunk
7. Descending aorta
1.3.9 Case 9
A 64-year-old female patient with a neuroendocrine tumor in the pancreatic tail. Selected SPECT (top) and SPECT/CT (bottom) images of the upper abdomen with 111In-octreotide showed a focal area of slightly increased activity in the pancreatic tail. No other lesions were observed (Fig. 13) [27].
Fig. 13
111In-octreotide SPECT/CT
1.3.10 Case 10
A 41-year-old male patient with a history of carcinoid tumor, who attended for a regular check-up. 111In-octreotide SPECT/CT was done, finding focal increased activity in the middle to lower abdomen corresponding to mesenteric lymph node metastases, as well as in two metastatic lesions in the right hepatic lobe (Fig. 14) [30].
Fig. 14
111In-octreotide SPECT/CT
1.3.11 Case 11
A 39-year-old male patient with biopsy-proven lung carcinoid, who underwent 111In-octreotide SPECT/CT for staging. Images showed focal increased activity in the right hilum at the primary tumor, without definite uptake in post-obstructive atelectasis (Fig. 15) [32].
Fig. 15
111In-octreotide SPECT/CT
1.3.12 Case 12
A 51-year-old female patient with a biopsy confirmed diagnosis of transverse colon neuroendocrine tumor. 111In-octreotide SPECT/CT was performed for staging, finding only focal increased uptake in the primary lesion at the proximal transverse colon (Fig. 16) [33].
Fig. 16
111In-octreotide SPECT/CT
1.4 Neuroblastoma
1.4.1 Case 1
A 3-year-old girl with confirmed diagnosis of retroperitoneal neuroblastoma. 123I-MIBG SPECT/CT was performed for further evaluation. Images showed focal increased uptake in a retroperitoneal mass adjacent to the left psoas muscle, corresponding to the primary tumor. Neuroblastoma is a neural crest cell tumor arising from the sympathetic chain, commonly in the adrenal gland, and the mean age at the diagnosis was 2 years. Metastases may be found in 75% of these patients. Meta-iodobenzylguanidine (MIBG) is similar to norepinephrine and is taken up by chromaffin granules that are in neuroblastoma and pheochromocytoma (Fig. 17) [35].
Fig. 17
123I-MIBG SPECT/CT
1.5 Paraganglioma
1.5.1 Case 1
A 59-year-old male patient, who attended with hypertension and perspiration. Elevated levels of urinary catecholamines were found, so 123I-MIBG SPECT/CT was done for further evaluation. Images showed focal increased activity in a retroperitoneal mass at the aortocaval space, as well as in the left kidney superior pole. The surgical diagnosis confirmed a primary renal paraganglioma with retroperitoneal metastasis (Fig. 18).
Fig. 18
1. Abdominal aorta
2. Metastatic paraganglioma in aortocaval area
3. IVC
4. Right kidney
5. Liver, left lobe
6. Pancreas
7. Stomach
8. Renal paraganglioma
1.5.2 Case 2
A 57-year-old female patient with a history of left adrenal paraganglioma, who attended for routine check-up. 123I-MIBG SPECT/CT was performed, showing heterogeneous activity in the liver, with a focal nodular increased uptake in segment 5 (V). Heterogeneous activity in the liver is physiologic and related to timing of the imaging and radiotracer metabolism and excretion through the biliary system. However, focal increased uptake is an abnormal finding, and in this case, it corresponded to a metastatic lesion. Also, an active metastasis was found in the T8 vertebral body (Fig. 19) [36].
Fig. 19
123I-MIBG SPECT/CT
1.6 Thyroid Cancer
1.6.1 Case 1
A 59-year-old male patient with a history of thyroid cancer, who underwent coronary CT, finding incidentally multiple lung nodules. 131I SPECT/CT showed moderately to intense increased iodine uptake in the nodules, confirming metastatic disease. Iodine therapy with 200 mCi of 131I was administered (Figs. 20, 21, 22 and 23) [37].
Fig. 20
1. Lung metastases
2. Physiologic colonic uptake
Fig. 21
1. Thyroid bed
2. Left neck, level VI
3. Left sternocleidomastoid muscle
4. Left neck, level IV
Fig. 22
1. Right middle lobe (RML) anterior segment metastatic nodule
2. Right lung minor fissure
3. Right lung major fissure
4. Right bronchus intermedius
5. Right lower lobe (RLL) superior segment metastatic nodule
Fig. 23
1. Left lower lung lobe superior segment metastatic nodule
2. Left lower lung lobe lateral basal segment metastatic nodule
1.6.2 Case 2
A 34-year-old female patient with thyroid cancer, who underwent total thyroidectomy with central neck dissection. On 131I ablation scan, bone metastaseswere found, which were treated with 250 mCi of 131I. Post-treatment iodine scan and SPECT/CT were taken, showing intense focal iodine uptakes at T4 and T6, confirming iodine-avid bone metastases (Figs. 24, 25, 26, 27, 28, and 29) [38].
Fig. 24
1. Submandibular glands
2. Body of mandible
3. Genioglossus
4. Trachea
5. Sternocleidomastoid muscle
6. C2 spine
7. Obliquus capitis inferior muscle
Fig. 25
1. Right scapula
2. Right lung apex
3. Right subclavian artery
4. Right clavicle
5. Right common carotid artery
6. Trachea
7. Left internal jugular vein
8. Left subclavian vein
9. T2 spine
Fig. 26
1. Lung
2. Breast
3. Superior vena cava
4. Ascending aorta
5. Left pulmonary artery
6. Left fourth rib
7. Vertebral arch of T4 spine (metastasis)
Fig. 27
1. Lung parenchyma
2. Right fourth rib
3. Right atrium
4. Sternum
5. Left breast parenchyma
6. Left ventricle
7. Descending aorta
8. Vertebral body of T6 (metastasis)
Fig. 28
1. Liver
2. Descending aorta
3. Transverse colon
4. Stomach
5. Diaphragm
Fig. 29
1. Right kidney
2. Liver
3. Inferior vena cava
4. Transverse colon
5. Body of pancreas
6. Descending aorta
7. Jejunum
8. Left kidney
9. Spleen
1.6.3 Case 3
A 62-year-old female patient with thyroid cancer history, who was treated with thyroidectomy 6 months earlier. She attended a routine follow-up without symptoms and normal serum levels of thyroglobulin. Selected SPECT (top) and SPECT/CT (bottom) with 131I demonstrated a focal area of moderately increased activity in the left thyroid bed, which was confirmed to be residual functioning thyroid tissue (Fig. 30).
Fig. 30
131I SPECT/CT
1.7 Parathyroid Adenoma
1.7.1 Case 1
A 63-year-old male patient with hypercalcemia and weight loss. Laboratory tests showed abnormal serum calcium, phosphorus, and parathyroid hormone levels, so primary hyperparathyroidism was suspected. 99mTc-MIBI SPECT/CT was performed finding focal delayed uptake in the lower aspect of the right thyroid lobe, corresponding to a parathyroid adenoma, type E (Figs. 31, 32, 33, 34, and 35) [40, 41].
Fig. 31
1. Posterior arch of C1 spine
2. Parotid glands
3. Mandibular ramus
4. Pharyngeal space
5. Body of mandible
6. Body of tongue
7. Palatine tonsil
8. Masseter muscle (superficial part)
9. Trapezius muscle
10. Spinal cord
Fig. 32
1. Submandibular glands
2. Body of hyoid bone
3. Digastric muscle anterior belly
4. Epiglottis
Fig. 33
1. Internal jugular vein
2. Trapezius muscle
3. External jugular vein
4. Common carotid artery
5. Thyroid gland
6. Trachea
Fig. 34
1. Right common carotid artery
2. Parathyroid gland
3. Trachea
4. Thyroid Left lobe
5. Left clavicle
6. Left scapular
7. Head of left humerus
8. Left lung apex
9. Esophagus
Fig. 35
1. Right pectoralis major muscle
2. Subclavian artery
3. Common carotid artery
4. Sternum
5. Trachea
6. Humeral shaft
7. Scapular
8. Left Lung
9. Esophagus
10. Spinous process of T3 spine
1.7.2 Case 2
A 63-year-old female patient with suspicion of parathyroid adenoma, who underwent 99mTc-MIBI SPECT/CT. Images showed a focal area of moderately increased activity in the right lower anterior mediastinum, which was confirmed as a parathyroid adenoma, type F (Fig. 36) [42].
Fig. 36
99mTc-MIBI SPECT/CT
1.7.3 Case 3
A 71-year-old female patient with primary hyperparathyroidism, who underwent 99mTc-MIBI SPECT/CT. Images showed a focal moderately increased activity in the right paraesophageal area at the level of the thoracic inlet, which corresponded to a parathyroid adenoma, type F (Fig. 37) [42].
Fig. 37
99mTc-MIBI SPECT/CT
1.7.4 Case 4
A 56-year-old male patient with confirmed diagnosis of a parathyroid adenoma (type E). Selected SPECT (top) and SPECT/CT (bottom) of the neck and chest with 99mTc-MIBI were performed. Images showed a focal moderately increased activity in the right paratracheal area at the level of the right inferior thyroid bed (Fig. 38) [42].
Fig. 38
99mTc-MIBI SPECT/CT
1.7.5 Case 5
A 63-year-old female patient with suspicion of a parathyroid adenoma (type C). Selected SPECT (top) and SPECT/CT images of the neck and chest with 99mTc-MIBI showed a focal moderately increased activity in the right paraesophageal area, confirming the diagnosis (Fig. 39) [42].
Fig. 39
99mTc-MIBI SPECT/CT
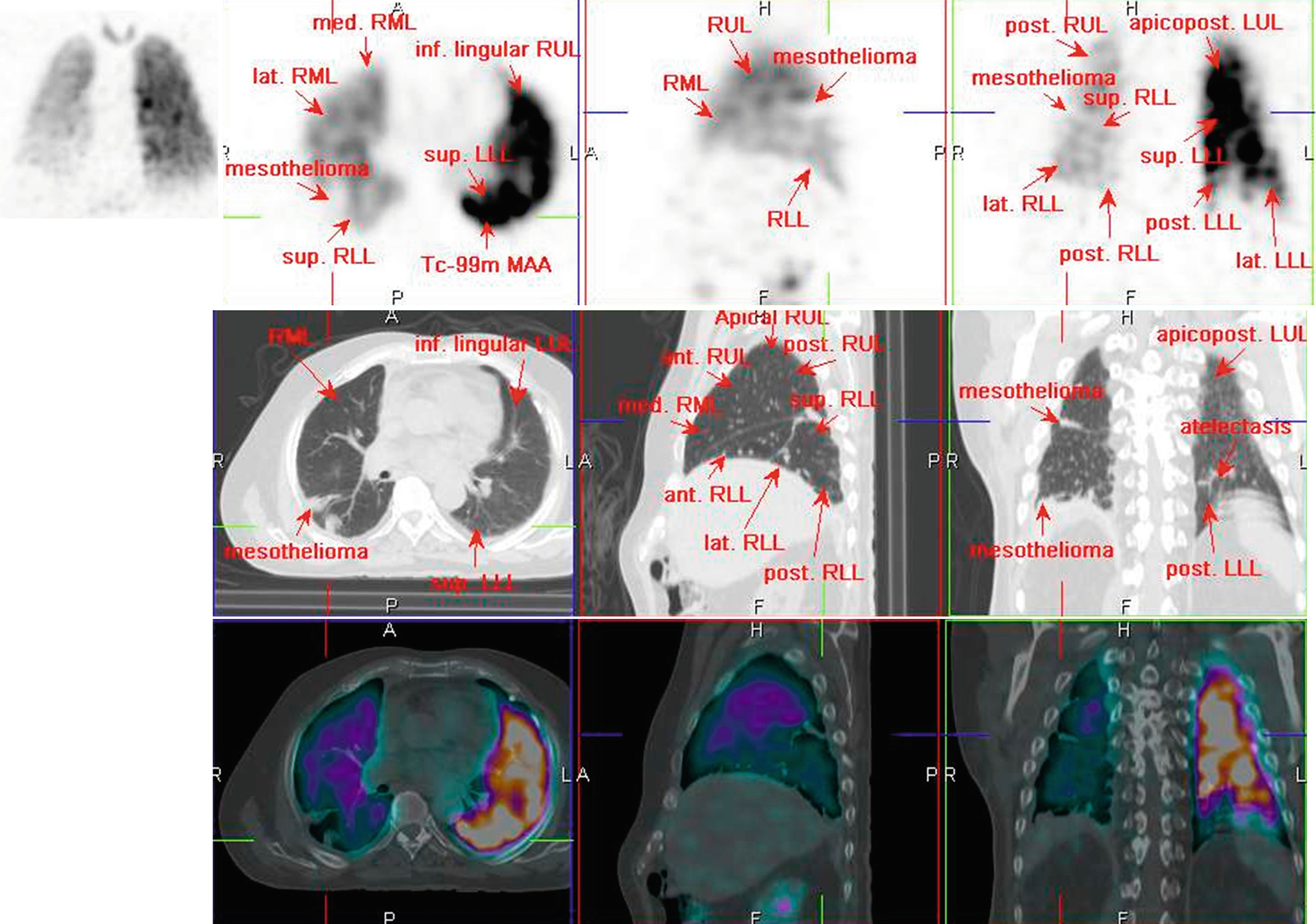
1.8 Mesothelioma
1.8.1 Case 1
A 69-year-old male patient with chest pain and dyspnea. The diagnosis of a mesothelioma was confirmed and 99mTc-MAA SPECT/CT was performed during staging. Images showed slightly decreased activity in the right upper and middle lobes as well as moderately decreased activity in the right lower lobe. Also noted were perfusion defects along the posterolateral periphery of the right lower lobe owing to nodular pleural lesions (Fig. 40) [43].
Fig. 40
99mTc-MAA SPECT/CT
1.9 Bone Tumors
1.9.1 Case 1
A 10-year-old girl with a history of ossifying fibroma, who underwent 99mTc-methylene diphosphonate (MDP) SPECT/CT during a follow-up. Images showed moderately increased activity in the bilateral maxillary sinuses and right mandible at expansile bone lesions with fibrous matrix and peripheral sclerotic rim. Ossifying fibromas are benign bone tumors and occur often in children under 10 years in the tibia, femur, mandible, maxilla, and nasal areas (Fig. 41) [45].
Fig. 41
99mTc-MDP SPECT/CT
1.9.2 Case 2
A 76-year-old male patient with lower back pain. 99mTc-MDP SPECT/CT showed focal increased uptake at bilateral L5-S1 facet joints, with degenerative changes. Additionally, a focal increased uptake was noted at the superior aspect of the left iliac bone, corresponding to a non-aggressive bone lesion with a central hipodense nidus surrounded by sclerotic bone changes, which was confirmed to be an osteoid osteoma (Fig. 42).
Only gold members can continue reading. Log In or Register to continue