Ankle
Anthony Wilson
John H. Harris Jr.
GENERAL CONSIDERATIONS
The ankle includes the distal end of the tibia, the fibula, and the talus. The medial and lateral malleoli, together with the horizontal plate of the distal articulating surface of the tibia, constitute the ankle mortise that receives the dome-shaped superior articulating surface of the talus. Although the talus is intimately involved in the ankle joint, it is one of the tarsal bones, and primary injuries of the talus are discussed in Chapter 22, Foot and Heel. Only those talar injuries associated with primary injuries of the ankle are discussed in this chapter.
The radiographic evaluation of acute lesions of the ankle requires accurate clinical assessment of the site of the injury. Conditions affecting the heel and foot, which may produce symptoms referable to “the ankle,” may not be recorded on ankle views and, thus, may be overlooked. The foot, heel, and ankle are distinct anatomic regions. Logically, then, each region requires particular radiographic projections that are usually inappropriate for the proper radiographic examination of the adjacent anatomic region.
Acknowledgement of the basic ligamentous anatomy of the ankle is fundamental to an understanding of the pathophysiology of ankle injuries and the clinical significance of the radiographic appearance of the skeletal injuries.
Ligamentous Anatomy
Laterally (Fig. 21.1), the anterior and posterior talofibular ligaments, together with the calcaneo-fibular ligament, constitute the lateral collateral ligament. The anterior and posterior talofibular ligaments extend horizontally from the anterior and posterior cortical surfaces of the fibula to the talus. The calcaneofibular ligaments extend inferoposteriorly from the tip of the lateral malleolus to the lateral surface of the body of the os calcis.
The medial collateral deltoid ligament (Fig. 21.2) is stronger and denser than the lateral collateral ligament and consists of superficial and deep fibers loosely arranged into three groups. These groups extend from the lateral malleolus to the tarsal navicular, the sustentaculum tali of the os calcis, and the talus.
Distally, the tibia and fibula are united by the anterior and posterior tibiofibular ligaments; the interosseous ligament, which is the distal extension of the interosseous membrane; and the interosseous membrane itself (Fig. 21.3). Even from this brief description, it must be apparent that the ligaments of the ankle are integral to the anatomy of the ankle joint. The presence of specific ligamentous injury about the ankle is deducible from the location and orientation of malleolar fractures. Identification of the disrupted and intact ligaments should be included as part of the radiologic report of ankle injuries.
RADIOGRAPHIC EXAMINATION
The routine radiographic examination of the ankle should include anteroposterior (AP), “mortise” internally rotated oblique, and lateral projections (Fig. 21.4), unless the patient’s condition
dictates a more limited AP and lateral examination. Oblique views, as included in the routine radiographic examination, can be useful in identifying minimally displaced fractures that are frequently identified or confirmed only by these projections (Figs. 21.5 and 21.6).
dictates a more limited AP and lateral examination. Oblique views, as included in the routine radiographic examination, can be useful in identifying minimally displaced fractures that are frequently identified or confirmed only by these projections (Figs. 21.5 and 21.6).
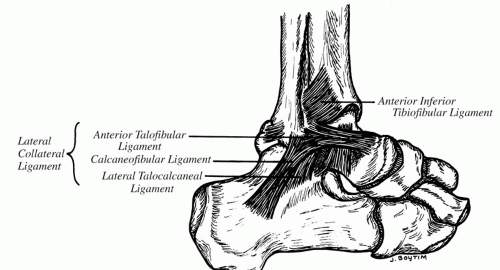 Figure 21.1. Schematic representation of the lateral collateral ligament of the ankle. |
The oblique projections of the ankle are obtained by rotation at the hip because rotation is not a physiologic function of either the ankle or the knee. The internally rotated oblique projection (e.g., the mortise view) requires only approximately 10 degrees of internal rotation at the hip or sufficient internal rotation so that the lateral malleolus is on the
same horizontal plane as the medial malleolus and both are parallel to the x-ray tabletop. The mortise view is the true AP projection of the ankle joint. Oblique projections,1 plain radiograph tomography (Fig. 21.7), computed tomography (CT), or magnetic resonance imaging (MRI) may be required to identify minimally displaced ankle fractures.
same horizontal plane as the medial malleolus and both are parallel to the x-ray tabletop. The mortise view is the true AP projection of the ankle joint. Oblique projections,1 plain radiograph tomography (Fig. 21.7), computed tomography (CT), or magnetic resonance imaging (MRI) may be required to identify minimally displaced ankle fractures.
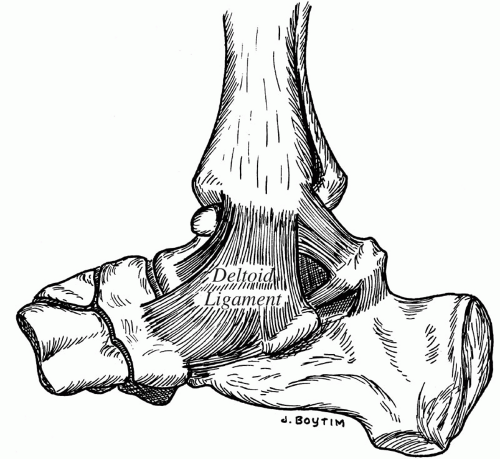 Figure 21.2. Schematic representation of the medial collateral (deltoid) ligament of the ankle. |
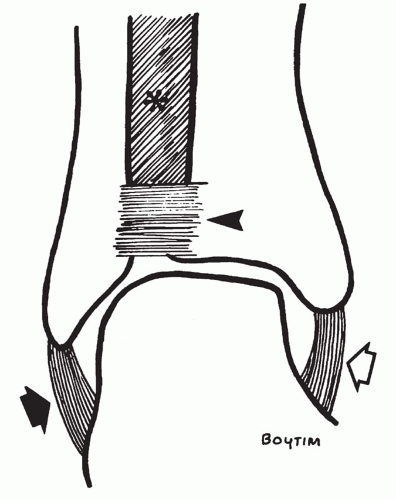 Figure 21.3. Schematic representation of the major ligaments of the ankle seen from the front. Asterisk indicates the interosseous ligament, the anterior tibiofibular ligament (arrowhead), the medial collateral or deltoid ligament (white arrow), and the lateral collateral ligament (black arrow). |
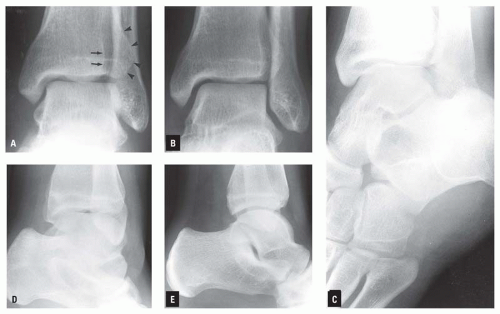 Figure 21.4. Routine radiographic examination of the ankle comprising straight AP (A), “mortise” (B), internally rotated oblique (C), externally rotated oblique (D), and lateral (E) projections. In the straight frontal projection (A), the arrows indicate the posterior margin, and the arrowheads, the anterior margin of the fibular notch of the lateral aspect of the tibia. |
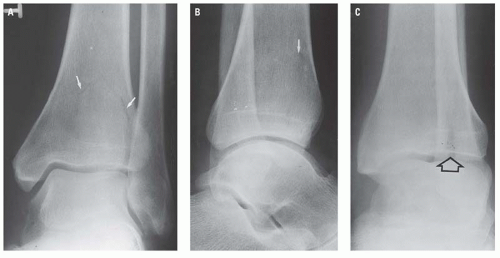 Figure 21.5. Subtle, minimally displaced fracture in the distal tibia. The fracture line is only faintly perceptible in the frontal (A) and lateral (B) projections (white arrows) but is clearly evident in the externally rotated oblique projection (C, open arrow). |
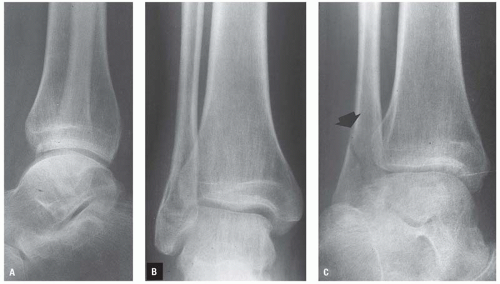 Figure 21.6. The minimally displaced fracture in the lateral malleolus (C, arrow) (eversion injury) is difficult to identify in the lateral (A) and frontal (B) projections and, consequently, could be overlooked. The fracture line is clearly perceptible in the internally rotated oblique projection (C). |
RADIOGRAPHIC ANATOMY
The osseous and ligamentous anatomy of the ankle is described and illustrated earlier. It is important to remember that the ankle mortise is composed not only of the malleoli and horizontal plate of the distal articulating surface of the tibia plafond, but also of the very important ligamentous structures that are not visible on plain radiographs.
In the straight AP view of the ankle, the lateral malleolus, lying slightly posterior in the fibular notch of the lateral aspect of the distal end of the tibia, is superimposed on the lateral aspect of the body of the talus. In this projection, therefore, the talofibular joint space cannot be adequately evaluated. The need to visualize the talofibular space and to be able to compare it with the talotibial medial space, to obtain an unobstructed view of the lateral margin of the talar trochlea dome, and to determine the relationship of the proximal talar articulating surface to the plafond have all prompted the routine use of the mortise view. In this projection, the lateral surface of the talar body and the cortex of the posterior margin of the fibular notch should normally be on approximately the same vertical plane (Fig. 21.4B). In the lateral projection (Fig. 21.4C), the concavity of the distal tibial articulating surface and the convexity of the talar trochlea are normally congruous.
The optimum lateral radiograph of the ankle results when the part is positioned so that the malleoli are directly superimposed on each other (Fig. 21.4C). This view should include the entire os calcis and the bones of the midfoot, including the base of the fifth metatarsal. Although neither the calcaneus nor the fifth metatarsal is a component of the ankle, each must be consciously studied for the presence of a fracture that may have been clinically interpreted as an injury to the ankle. For this reason, it is particularly important that the base of the fifth
metatarsal be included in all radiographic examinations of the ankle. Fracture of the base of the fifth metatarsal (Fig. 21.8) is commonly misdiagnosed as an ankle fracture clinically, and the patient referred for radiographic examination of the ankle. In these circumstances, if the midfoot is not included on the ankle examination, the fifth metatarsal fracture could be missed.
metatarsal be included in all radiographic examinations of the ankle. Fracture of the base of the fifth metatarsal (Fig. 21.8) is commonly misdiagnosed as an ankle fracture clinically, and the patient referred for radiographic examination of the ankle. In these circumstances, if the midfoot is not included on the ankle examination, the fifth metatarsal fracture could be missed.
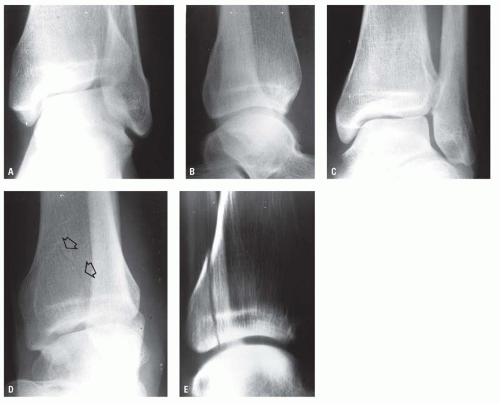 Figure 21.7. Minimally displaced posterior tibial lip fracture is not visible on the frontal, lateral, or mortice views (A-C) and is suggested only in the externally rotated oblique projection (D, open arrows) and is confirmed by plain radiographic tomography (E). |
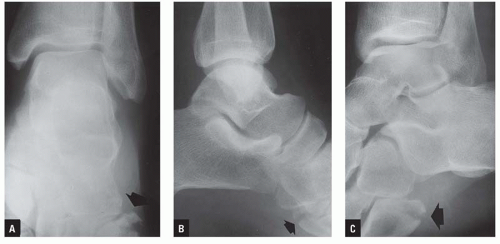 Figure 21.8. The frontal projection of the ankle (A) is negative. However, a comminuted, displaced fracture of the base of the fifth metatarsal (arrow) is visible at the edge of the radiograph. The fracture of the base of the fifth metatarsal (arrow) can be seen in the lateral projection of the ankle (B) but is seen to best advantage in the internally rotated oblique projection (C). |
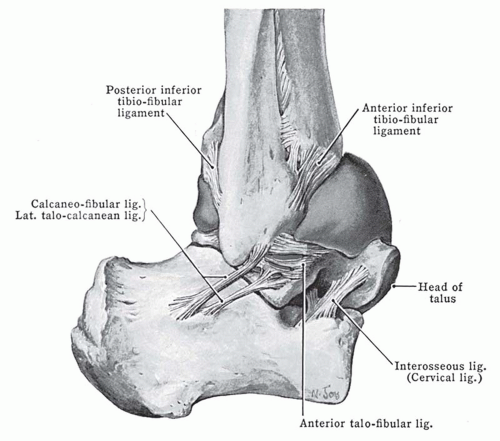 Figure 21.9. Note the anterior bulge of the distended capsule of the ankle joint. (From Anderson JE. Grant’s Atlas of Anatomy. 6th ed. Baltimore, MD: Williams & Wilkins; 1972, used with permission.) |
The articular capsule of the ankle surrounds the joint. It is attached to the margin of the distal tibial articulating surface, the malleoli, and extends distally to attach onto the neck of the talus. Laterally, the capsule attaches on the fibula near the lateral malleolar fossa (Fig. 21.9).2 Thus, posttraumatic distention of the ankle joint capsule, which may be visible on a properly exposed lateral ankle radiograph (Fig. 21.10), should be considered indicative of an intra-articular fracture of the distal tibia, the malleoli, or the talar body until specifically excluded by any of the appropriate imaging modalities, including MRI.
The radiographic appearance of the normal child’s ankle is seen in Figure 21.11. The distal tibial epiphysis appears during the 2nd year of life and fuses in the
18th year. The distal fibular epiphysis appears at age 2 and fuses at age 20. Infrequently, the tip of the medial malleolus arises from a separate ossification center. The radiographic characteristics of this apophysis, its relationship to the epiphysis, and its frequent bilaterality help distinguish this normal variant from an avulsion fracture fragment (Fig. 21.12).
18th year. The distal fibular epiphysis appears at age 2 and fuses at age 20. Infrequently, the tip of the medial malleolus arises from a separate ossification center. The radiographic characteristics of this apophysis, its relationship to the epiphysis, and its frequent bilaterality help distinguish this normal variant from an avulsion fracture fragment (Fig. 21.12).
 Figure 21.10. Distended ankle joint capsule (solid arrows) in an adolescent with a minimally displaced physeal injury (open arrow). |
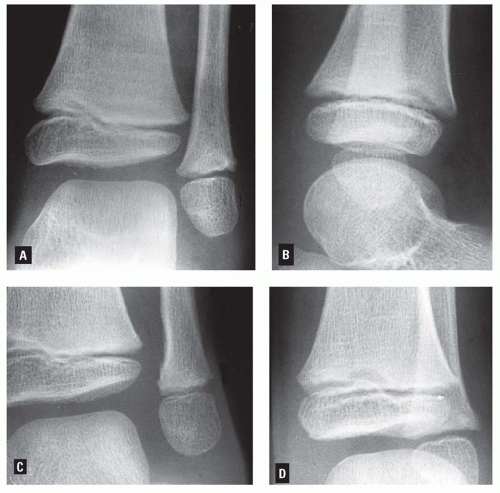 Figure 21.11. Radiographic appearance of the normal ankle of a 5-year-old boy in AP (A), lateral (B), and internally (C) and externally (D) rotated projections. The normal vagaries of the surfaces of the physes may simulate physeal injury or fracture. In that event, frontal and lateral radiographs of the opposite side should be obtained for comparison purposes. |
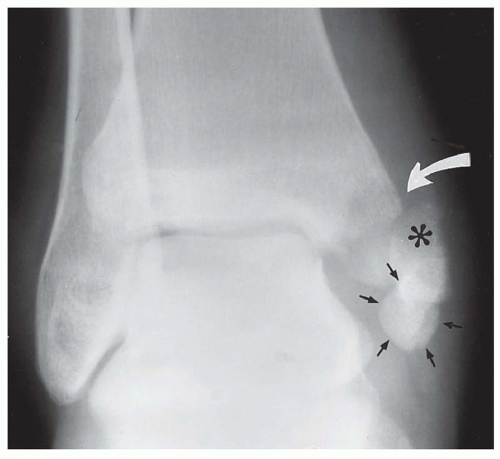 Figure 21.12. This patient sustained a comminuted fracture (curved arrow) of the medial malleolus secondary to direct blunt trauma. The smoothly corticated round ossicle (small arrows) distal to the large distal malleolar fragment (asterisk) represents an ununited secondary ossification center of the medial malleolar styloid process. The difference in its radiographic characteristics compared with those of the more proximal fracture fragments distinguishes it from the fracture fragments. |
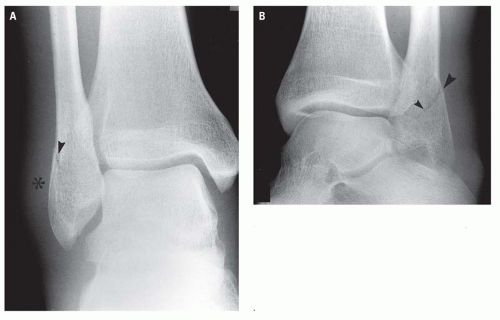 Figure 21.13. Eversion injury of the right ankle in which diffuse soft tissue swelling (asterisk) along the lateral aspect of the ankle (A) is the most obvious radiologic sign of the minimally displaced oblique fracture of the lateral malleolus (arrowheads), seen best in the oblique radiograph (B). |
RADIOGRAPHIC MANIFESTATIONS OF TRAUMA
Extracapsular soft tissue swelling about the ankle joint is discernible in a properly exposed radiograph. Although this is a nonspecific finding and is frequently present without associated skeletal trauma, it may signal a subtle fracture (Fig. 21.13). The radiographic distinction between extra-articular soft tissue swelling and joint capsular distention and its significant posttrauma is shown in Figure 21.14.
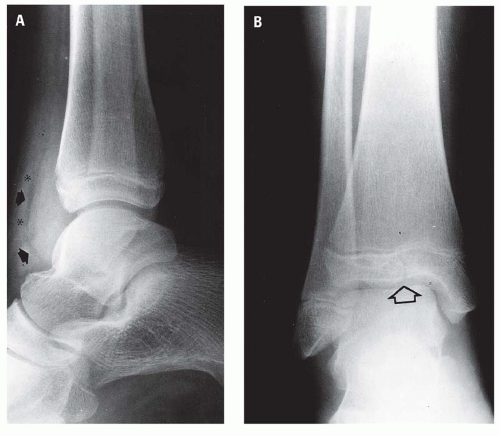 Figure 21.14. A: In the lateral projection, the closed arrows indicate the anterior bulge of the distended joint capsule, and the asterisks indicate the extracapsular soft tissue swelling. B: In the frontal projection, there is minor separation of the lateral portion of the distal tibial physis, and the open arrow indicates the subtle Salter-Harris III distal tibial epiphyseal-physeal injury. |
Physeal Injuries
Epiphyseal-physeal injuries, which commonly involve the ankle, are designated according to the Salter-Harris classification (Table 21.1).3, 4 The distal tibial
epiphysis is the single most common site of physeal injury.5 Types III and IV occur more commonly at the ankle than at any other site.
epiphysis is the single most common site of physeal injury.5 Types III and IV occur more commonly at the ankle than at any other site.
TABLE 21.1 Salter-Harris Classification of Physeal Injuries | ||
|---|---|---|
|
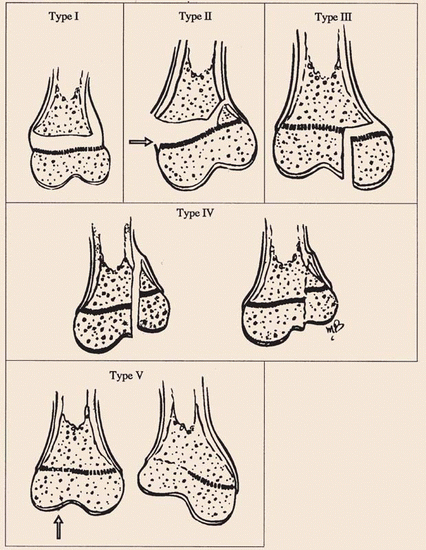
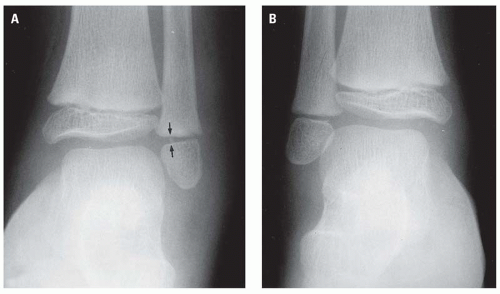 Figure 21.15. A: Salter-Harris type I physeal injury of the distal left fibula. As defined, the distal fibular metaphysis and epiphysis are intact. The injury is recognized by the soft tissue swelling lateral to the lateral malleolus and the lack of parallelism of the metaphyseal and epiphyseal margins of the physis (e.g., medial widening of the distal fibular physis) (arrows). B: Normal right ankle for comparison. Note that the metaphyseal and epiphyseal margins of the physis of the normal ankle are congruous. |
Type I epiphyseal injury, which occurs most commonly in young children, was originally described by Salter as being an epiphyseal separation without a metaphyseal or epiphyseal fracture. Typically, the momentarily separated epiphysis returns to an anatomic or type position with respect to the adjacent metaphysis by the intact periosteum. For this reason, the type I physeal injury is difficult to recognize radiographically. The most striking radiographic sign of type I injury is soft tissue swelling adjacent to the physis and minor uniform or eccentric widening of the physis itself (Figs. 21.15 and 21.16). In displaced type I physeal injuries, the periosteum is attenuated or disrupted, permitting epiphyseal displacement. The periosteum is usually disrupted on the convex side while remaining intact on the concave side of the epiphyseal displacement. Occasionally, a tiny fragment of bone is pulled off the margin of the metaphyseal or epiphyseal surface of the physis. The presence of such a fragment, usually situated in the lateral aspect of the physis between the metaphyseal and epiphyseal surfaces, together with widening of the physis and adjacent soft tissue swelling, establishes a type I physeal injury (Fig. 21.17). This tiny avulsion fracture fragment, although not included in the original Salter-Harris classification, is very commonly visible and is very helpful in the
radiologic identification of the type I physeal injury. The tiny separate fragment has none of the characteristics of the metaphyseal component of the type II physeal injury. Consequently, it seems reasonable to include this type of avulsion fracture as a variant of the type I injury.
radiologic identification of the type I physeal injury. The tiny separate fragment has none of the characteristics of the metaphyseal component of the type II physeal injury. Consequently, it seems reasonable to include this type of avulsion fracture as a variant of the type I injury.
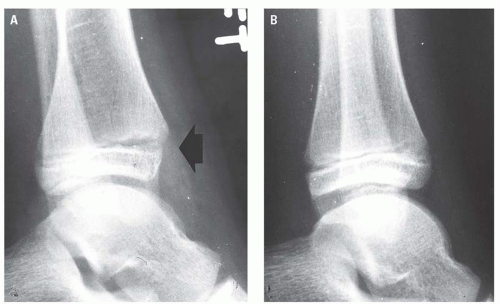 Figure 21.16. A: Salter-Harris type I distal tibial physeal injury. The physis is widened anteriorly and narrowed posteriorly, and consequently the epiphysis is eccentrically situated with respect to the adjacent metaphysis (arrow). B: The normal side has been reversed for ease of comparison. |
Type II physeal injury consists of an oblique fracture extending through the metaphysis into the physis with separation through the remainder of the physis. The triangular metaphyseal fragment, together with the intact epiphysis, constitutes the distal fragment of the type II injury (Fig. 21.18). The type II injury is by far the most common of the physeal injuries and usually occurs in older children. The prognosis for normal growth is excellent. Type II injuries of the ankle are usually obvious radiographically but may be subtle and not discernible on all ankle views (Fig. 21.19).
Physeal injuries are limited to a single bone but may also be associated with a fracture (Fig. 21.20) or physeal injury of an adjacent bone.
Physeal injuries are limited to a single bone but may also be associated with a fracture (Fig. 21.20) or physeal injury of an adjacent bone.
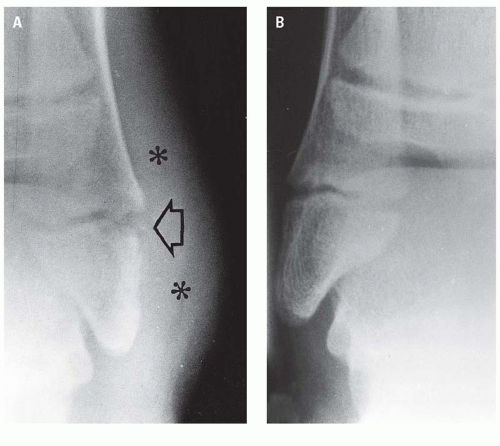 Figure 21.17. A: Salter-Harris type I distal fibular physeal injury on the left. The physis is widened laterally, and a tiny fracture fragment (open arrow) has been pulled from the lateral margin of the physis. Diffuse soft tissue swelling (asterisks) is present about the lateral malleolus. B: Normal right ankle for comparison. |
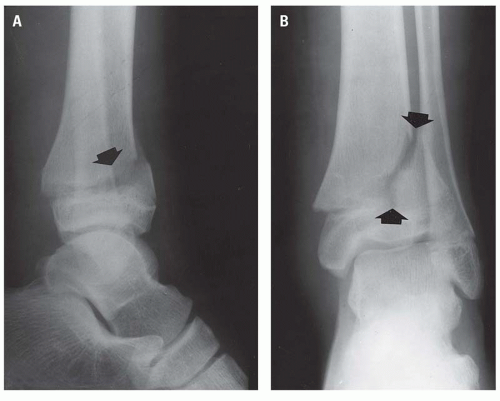 Figure 21.18. Salter-Harris type II distal tibial physeal injury. Arrows indicate the metaphyseal fracture in both lateral (A) and AP (B) projections. Note that the resultant triangular metaphyseal fragment is normally related to the epiphysis. The epiphysis, together with the triangular metaphyseal fragment, has been separated medially and posteriorly and is displaced anteriorly and laterally relative to the remainder of the metaphysis. |
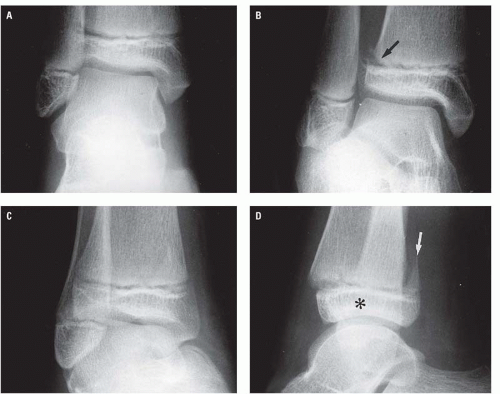 Figure 21.19. Subtle Salter-Harris type II physeal injury of the distal tibia not visible in the frontal (A) projection is evidenced only by the minor disruption of the lateral aspect of the tibial metaphysis (arrow) in the mortise view (B). This diagnosis is established only in the lateral radiograph (C), where posterior displacement of the epiphysis (asterisk) and attached posterior metaphyseal fragment (arrow) is clearly evident (D). |
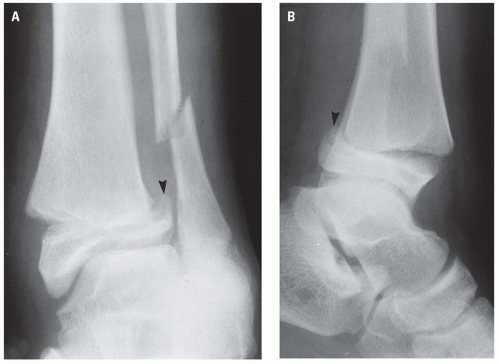 Figure 21.20. Salter-Harris type II distal tibial injury associated with a distal third fibular fracture in an eversion injury of the ankle. The metaphyseal component (arrowhead) is evident in both frontal (A) and lateral (B) projections. |
Type III injury is uncommon, is usually seen in the distal tibial epiphysis, and is entirely intracapsular. The prognosis of normal growth is good, provided the blood supply to the separated portion of the epiphysis has not been disrupted. Radiographically, the injury consists of a vertical fracture line that extends perpendicularly through the epiphysis from its articulating surface to the physis and then along the physis to its margin. Figure 21.21 illustrates a minimally displaced Salter-Harris III physeal injury in a very young child.
The biplane fracture of Tillaux6 (Fig. 21.22) is a variant of the type III injury of the distal tibial epiphysis. The vertical epiphyseal fracture, situated in the lateral aspect of the epiphysis, occurs in older children in whom fusion of the medial portion of the distal tibial physis is more advanced than the lateral (Fig. 21.23). The mechanism of injury has been described as eversion or external rotation. The epiphyseal injury is an avulsion fracture produced by the intact anterior and posterior tibiofibular ligaments. The age of the patient usually 12 to 14 years, radiographic evidence of fusion of the medial portion of the distal tibial physis, and lateral displacement of the epiphyseal fragment distinguishes the biplane fracture of Tillaux (Fig. 21.24) from the typical type III injury of the distal tibial epiphysis.
The type IV and the rare type V physeal injuries differ in two significant aspects from the other Salter-Harris injuries, in that each is caused by a compressive rather than a shearing or rotational force and each has a high propensity for growth arrest secondary to premature or uneven physeal fusion. In both type IV and type V injuries, premature physeal closure may result from physical crushing of the physeal cells, impairment of their blood supply,
or damage to the metaphysis and epiphysis with the resultant formation.7 Additionally, peculiar to the type IV injury is growth arrest secondary to fusion of the epiphyseal component of the separate fragment to the metaphysis of the major fragment. This is described in more detail later.
or damage to the metaphysis and epiphysis with the resultant formation.7 Additionally, peculiar to the type IV injury is growth arrest secondary to fusion of the epiphyseal component of the separate fragment to the metaphysis of the major fragment. This is described in more detail later.
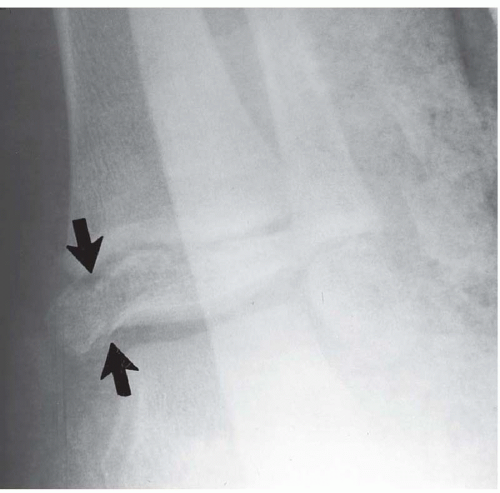 Figure 21.21. Salter-Harris type III injury of the distal tibial epiphysis (arrows) of an infant. |
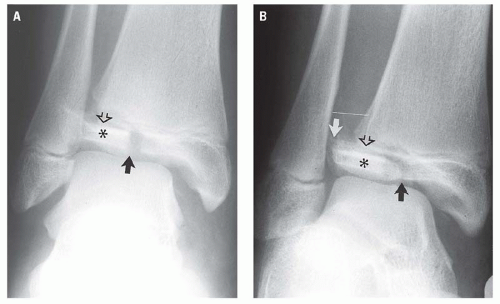 Figure 21.22. Classic biplanar fracture of Tillaux. In both the AP (A) and mortise (B) views, the vertical fracture of the epiphysis (black arrow) involves the junction of its lateral and middle thirds. The lateral aspect of the physis is disrupted (open arrow), and the separate epiphyseal fragment (asterisk) is avulsed laterally by the intact tibiofibular ligaments. The normal relationship between the laterally displaced fibula and epiphyseal fragment (B, white arrow) indicates that the tibiofibular ligaments are intact, while more proximally, the interosseous membrane can be reasonably assumed to be disrupted because of the distance between the fibular metaphysis and the superior portion of the fibular groove (B, white line). |
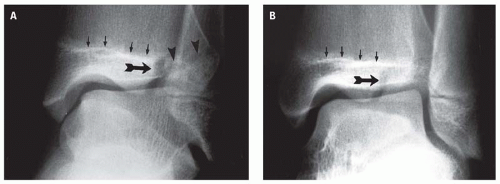 Figure 21.23. Biplane fracture of Tillaux in AP (A) and mortise (B) projections. The medial twothirds of the distal tibial physis is fused (small arrows). A vertical fracture (large arrow) is present in the lateral third of the epiphysis, and the physeal separation clearly extends to its lateral margin (arrowheads). |
Type IV injury consists of a vertical fracture extending through the entire thickness of the medial third of the distal tibial epiphysis, across the physis, and continuing vertically through the metaphysis to exit through the medial metaphyseal cortex (Fig. 21.25). The entire separate fragment, therefore, includes the
medial malleolus with variable amounts of the medial portion of the plafond, the physis, and the metaphysis as a single unit. The mechanism of injury is primarily axial-loading vertical compression and inversion of the foot, causing the talus to impact against the medial malleolus. Continued inversion and/or vertical compression causes proximal displacement of the separate fragment (Fig. 21.26). The vertical compression component invariably results in a Salter-Harris type V injury of the physis itself. If the separate fragment remains proximally displaced and assuming there is no other distal tibial physeal injury, growth arrest will occur as the result of the epiphyseal component fusing with the metaphysis of the major fragment (Fig. 21.26B,C). “Perfect” open reduction and internal fixation7, 8 offers the best chance of healing without growth arrest. However, as mentioned earlier and as seen in the patient represented in Figure 21.26, a crushing injury Salter-Harris type V concurrently involving the distal tibial physis will contribute in large measure to the premature closure of the distal tibial physis.
medial malleolus with variable amounts of the medial portion of the plafond, the physis, and the metaphysis as a single unit. The mechanism of injury is primarily axial-loading vertical compression and inversion of the foot, causing the talus to impact against the medial malleolus. Continued inversion and/or vertical compression causes proximal displacement of the separate fragment (Fig. 21.26). The vertical compression component invariably results in a Salter-Harris type V injury of the physis itself. If the separate fragment remains proximally displaced and assuming there is no other distal tibial physeal injury, growth arrest will occur as the result of the epiphyseal component fusing with the metaphysis of the major fragment (Fig. 21.26B,C). “Perfect” open reduction and internal fixation7, 8 offers the best chance of healing without growth arrest. However, as mentioned earlier and as seen in the patient represented in Figure 21.26, a crushing injury Salter-Harris type V concurrently involving the distal tibial physis will contribute in large measure to the premature closure of the distal tibial physis.
 Figure 21.24. Minimally displaced biplanar fracture of Tillaux (arrow). |
The “triplanar” fracture5, 9, 10 is a variant of the Salter-Harris type IV injury7 in that it includes a fracture of the epiphysis, separation of a portion of the physis, and a fracture through the distal tibial metaphysis, as does the type IV injury. The triplanar fracture differs
from the type IV in that the triplanar injury occurs in three planes, whereas the type IV occurs in only one. The sites of disruption of the triplanar fracture occur in the sagittal plane epiphysis, the axial plane physis, and the coronal plane metaphysis. Triplanar fractures may occur in a two-part variety, in which all the components of the separate fragment exist as an intact unit (Fig. 21.27), or in a three-part configuration (Fig. 21.28),5 in which the epiphyseal component is a separate fragment (e.g., the third part) (Fig. 21.29).
from the type IV in that the triplanar injury occurs in three planes, whereas the type IV occurs in only one. The sites of disruption of the triplanar fracture occur in the sagittal plane epiphysis, the axial plane physis, and the coronal plane metaphysis. Triplanar fractures may occur in a two-part variety, in which all the components of the separate fragment exist as an intact unit (Fig. 21.27), or in a three-part configuration (Fig. 21.28),5 in which the epiphyseal component is a separate fragment (e.g., the third part) (Fig. 21.29).
 Figure 21.25. Salter-Harris IV physeal injury (white arrows). Even the minimal superior displacement of the separate fragment (arrowhead) will permit the malleolar epiphyseal component to fuse with the distal tibial metaphysis (black arrow), resulting in arrested bone growth. In this patient, it is impossible to exclude a concomitant Salter-Harris V injury of the distal tibial physis or a Salter-Harris I of the distal fibular physis. |
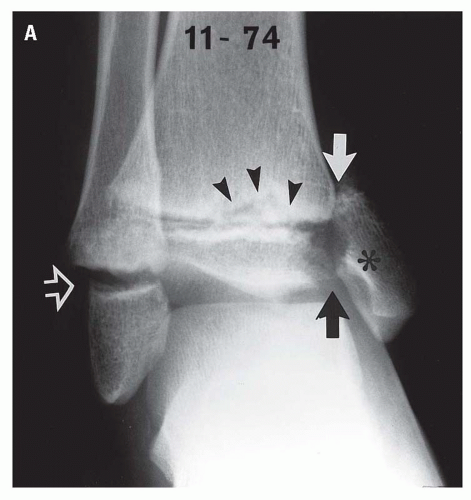 Figure 21.26. Concurrent type IV (closed arrows) and type V (arrowheads) distal tibial physeal and type I (open arrow) distal fibular physeal injuries, acutely (A) and over the ensuing 28 months (B,C). A: On the initial AP radiograph, the type IV fragment (asterisk) is proximally displaced. Buckling, irregularity, and sclerosis, particularly of the metaphyseal surface of the distal tibial physis (arrowheads), indicate the type V injury. (continued) |
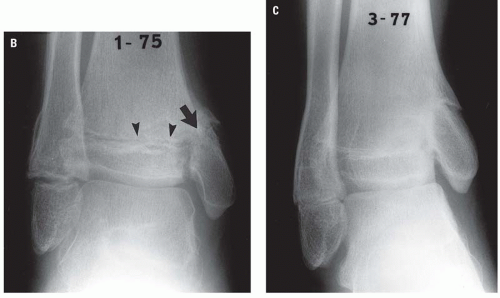 Figure 21.26. (continued) B: Within 2 months of the acute injury, the proximal portion of the medial malleolar epiphysis had fused with the metaphysis (arrow) of the major fragment, and signs of premature closure (arrowheads) of the remainder of the distal tibial physis are evident. C: At 28 months postinjury, the effects of distal tibial growth arrest and continued normal fibular growth are obvious. |
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


