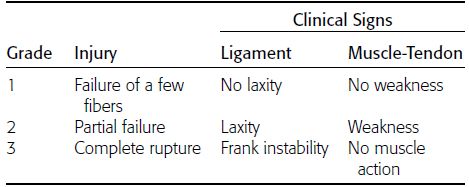
CHAPTER 1 Trauma to the human frame may cause deformation and breakage. The radiology of musculoskeletal trauma is more than a search for broken bones; it is an analysis of the effect of traumatic forces on a particular patient. It requires an understanding of the ways in which various forces affect the body: how they are applied, where they concentrate, and how they disrupt structural integrity. Fractures are but one manifestation of trauma; injuries to the soft tissues and other organ systems may be present. Fractures are not isolated phenomena; rather, they occur in the context of individual patients. Characteristics that affect the frequency, severity, location, and type of fracture include age, gender, activity, and health of the musculoskeletal system. The incidence of fractures of the extremities has a bimodal distribution with respect to age. In men, there is a first peak, between 10 and 20 years of age, which is related to immaturity of the skeleton, and a second peak, beginning at approximately 70 years of age, which is related to involutional osteoporosis. In women, there is a first peak at 10 years of age, again related to immaturity of the skeleton, and a second peak, beginning at approximately 50 years of age, that is related to postmenopausal osteoporosis. The skeleton is weak when it is growing, gains strength as it matures, and weakens again as it ages. Under 50 years of age, fractures are more common in males than in females because of greater exposure to trauma, but over 50 years of age, fractures in women become more common because of osteoporosis. In adolescents and young adults, the most common sites of fractures in the extremities are the phalanges and metacarpals of the hand, the distal humerus, the shaft of the tibia, the clavicle, the distal radius, and the phalanges of the foot. In adults older than 50 years of age, the most common sites of fractures in the extremities are the proximal femur, the proximal humerus, the distal radius, and the pelvis. Bone responds to trauma in predictable ways. From knowledge of the anatomic site involved and the forces applied, one can often predict the fractures that result. Conversely, knowing the site and morphology of a particular fracture frequently allows one to infer the forces that caused it. Such knowledge has practical applications to diagnosis and management. Application of external force to the bone is called loading. Bone is physically deformed (i.e., undergoes strain) when it is placed under a load (Fig. 1.1). At physiologic levels of loading, the bone undergoes elastic deformation as it absorbs and stores the energy imparted by the loading. When the load is removed, the stored energy is dissipated by elastic recoil, the bone recovers its preloaded shape, and no damage is sustained. Loading has a linear relationship to elastic deformation called stiffness. The stiffer the material, the less it deforms under a given load. When the severity of loading exceeds the level at which elastic recoil is possible, the bone sustains plastic (also called ductile) deformation. The absorbed energy from loading is expended in the work of permanently deforming the bone. The ductility of a material describes the degree to which it can sustain plastic deformation without breaking. At even greater levels of loading, the bone fails completely, and the imparted energy is expended in fracturing the bone and displacing the fragments. If loading continues, other body parts may sustain injury. Excessive loading results in injury; in general, the greater the amount of loading and the more rapidly it is applied, the more severe the injury. FIGURE 1.1. Various modes of loading. The external force of loading involves three fundamental components: compressive, tensile, and shear. The compressive component acts inwardly and squashes the bone together, the tensile component acts outwardly and pulls the bone apart, and the shear component acts parallel to the direction of force and sends different points in the bone past each other. The bone subjected to tensile loading tends to elongate; mechanical failure occurs when cement lines debond and the osteons are pulled apart. The bone subjected to compressive loading tends to shorten; mechanical failure occurs when individual osteons sustain oblique cracking. The bone subjected to shear loading undergoes angular deformity. Both tensile and compressive loadings have shear as a component because angular deformity occurs as the bone elongates or shortens. Bone is a diphasic material comprised of a rigid calcium hydroxyapatite crystalline structure that is resistant to compressive forces and a collagenous matrix of flexible fibrils and ground substance that is resistant to tensile forces. In compact bone (also referred to as lamellar bone or cortical bone), the material of bone is organized into concentric layers around the neurovascular supply to form osteons (haversian systems). Osteons are the basic functional and structural unit of compact bone. In cancellous bone (trabecular bone), the material of bone is organized into a three-dimensional latticelike system of plates and columns (trabeculae), with the neurovascular supply passing between trabeculae. Compact bone is stiffer than cancellous bone, but cancellous bone is more ductile. The functional architecture of mature bone reflects a continuing process of remodeling to accommodate the type, magnitude, and direction of physiologic loading. In general, bone resists compression better than tension and tension better than shear. Loading can be direct or indirect. Direct loading causes injuries at the site of loading. The morphology of fractures caused by direct loading—although related to the site, direction, and amount of force applied—tends to be unpredictable. Such injuries may be classified as crushing, penetrating, or tapping. A crushing injury results from the application of a large force over a large area, for example, a building collapsing on an individual. Crushing force results in comminuted or transverse fractures and extensive soft-tissue damage. A penetrating injury results from a large force being applied to a small area, for example, a gunshot wound. Penetrating force usually results in comminuted fractures; the degree of comminution depends on the energy of the penetrating projectile (Fig. 1.2). A tapping injury results from a small force being applied to a small area, for example, a blow to the forearm from a nightstick. Tapping force results in a transverse or stellate fracture at the site of impact (Fig. 1.3). Bones without much soft-tissue coverage, such as the ulna or tibia, are more vulnerable to direct trauma than bones such as the humerus or femur. FIGURE 1.2. Low-velocity gunshot wound causing comminuted fractures of the ulnar shaft. FIGURE 1.3. Tapping fracture of the ulnar shaft (nightstick fracture). Indirect loading causes injuries at a distance from the site of loading. The morphology of fractures caused by indirect loading tends to be predictable. Loading under tension (pulling apart), compression (squashing together), torsion (twisting), angulation (bending), and certain combinations of these produce fractures with predictable shapes that often occur at specific sites (Fig. 1.4). Soft tissues may modify indirect loading—for example, muscles can reduce tensile loads on bones by contracting and supplying an opposing compressive force. FIGURE 1.4. Types of loading correlated with direction of fracture lines. Traction or tension fractures occur as a result of traction on a bone by a tendon or ligament. The bone is pulled apart, or avulsed, and the fracture line is transverse to the direction of force as the bone fibers fail under tension. At the fingers, for example, fragments of bone may be avulsed at the insertions of tendons or ligaments (Fig. 1.5). The size of the avulsed fragment may range from large to tiny (Fig. 1.6). A large fragment may comprise a full-thickness piece of the bone; a small fragment may represent a mere fraction of the cortex. Tension fractures are most common in cancellous bone. FIGURE 1.5. Avulsion fragment at the extensor insertion at the distal phalanx (arrow). FIGURE 1.6. Tiny avulsion fragment at the volar plate attachment at the middle phalanx (arrow). When a long bone is angulated, the convex side is placed under tension, and the concave side is placed under compression. Because the bone fails first under tension, a transverse fracture propagates across the bone from the convex side. On the concave side, the bone may fail under compressive and shearing forces and splinter. Alternatively, a triangular fragment may shear off at an angle to the main fracture line. This results in comminution with a butterfly fragment on the concave side of the bend (Fig. 1.7). FIGURE 1.7. Transverse fracture of the tibia with butterfly fragment. Longitudinal compressive loading of the shaft of a long bone results in an oblique fracture caused by osteons being forced past each other and shearing off (Fig. 1.8). Compressive loading of a whole bone often results in T- or Y-shaped fractures as the hard cortical bone of the shaft is driven into the softer cancellous metaphysis. Such fractures are common at the ends of the humerus or femur and in the hands and toes. FIGURE 1.8. Oblique fracture of the proximal phalanx of the middle finger. Rotational loading (torsion or twisting) causes horizontal shearing with compressive and tensile components at an angle to the long axis of the shaft (Fig. 1.9). These stresses lead to a spiral fracture that curves around the circumference of the bone, representing a failure in tension, as the bone is pulled apart. The fracture line makes one complete rotation around the circumference of the bone and has sharp pointed ends joined by a vertical component (Fig. 1.10). The vertical fracture acts as a hinge, with the fracture fragments separating on the opposite side along the curved component. FIGURE 1.9. Diagrammatic representation of spiral fracture. On the near cortex of the bone, under torsion, horizontal shear stress forces points in the bone past each other. Tensile stress is present because these points are at the same time pulled apart, leading to an obliquely oriented tension fracture around the circumference of the bone. On the far cortex of the bone, compressive forces are present, leading to a vertical fracture that joins the spiral fracture lines. FIGURE 1.10. Spiral fracture of the tibial shaft. A: AP view. B: Lateral view. Many fractures are produced by a combination of forces. Angulation with axial compression results in a curved fracture line with oblique and transverse components and sometimes a butterfly fragment. Angulation with rotation results in an oblique fracture with short, blunted ends. Bone bruises are traumatic injuries to cancellous bone in which hemorrhage and edema displace the normal marrow. These injuries, which involve microfractures of individual trabeculae and disruption of small vessels, are evident on MRI as regions of localized edema with intact overlying articular cartilage and subcortical bone. The mechanism of injury is typically compression, either from direct impact or from indirect loading, with the impact transmitted through an adjacent bone. When the mechanism is direct impact, the bone bruise is usually isolated. When the mechanism is through indirect, transmitted impact, additional significant injuries may be present elsewhere in the anatomic region (Fig. 1.11). The pattern of bone bruises may help to identify associated injuries and suggest the mechanism of injury. Bone bruises typically revert to normal on follow-up MRI within several months; typically, the radiograph remains normal throughout the episode. FIGURE 1.11. Bone bruises caused by hyperextension injury. Sagittal T2-weighted fat-suppressed MRI shows a bone bruise in the anterior aspect of the lateral tibial plateau and a matching impaction fracture of the lateral femoral condyle. Although some fractures can be identified on virtually any imaging modality, radiography dominates the imaging evaluation for acute fractures. CT has a supporting role in characterizing complex fractures in preparation for possible surgery and occasionally in identifying fractures when radiographs are equivocal. In the spine, CT is used to screen for fractures in the setting of polytrauma. MRI may be used for identifying fractures, particularly stress and insufficiency fractures, when radiographs are negative or equivocal. MRI is more commonly used for identifying and characterizing soft-tissue and joint injuries. The radionuclide bone scan may be used for identifying stress fractures. Radiographs are a diagnostic supplement to the history and physical examination; care of the patient should not be secondary to performing the radiographic examination. Splinting an injured limb, for example, can alleviate pain without interfering with subsequent radiologic examinations. On radiographs, fractures of cortical bone are definitively recognized as focal discontinuities in the structure of bone, particularly when displacement is present. Impacted fractures of cortical bone may be recognized as focal alterations in the contour of the bone, typically an abrupt change in what should otherwise be a smooth contour. Compression fractures in cancellous bone may have a discontinuity in the cortex, a change in shape, a linear region of sclerosis, or any combination of these features. Avulsion fractures occur when tension on the attachment of a tendon, ligament, or capsule pulls off a fragment of bone. These fractures may be recognized as displaced fragments that may range in size from less than 1 mm in thickness to several centimeters. On CT scans, features of fractures are similar to those seen on radiography, but the ability to display the features is greatly enhanced by axial cross sections and multiplanar reconstructions (Fig. 1.12). FIGURE 1.12. Subtle hip fracture on CT. A: Axial CT scan shows subtle discontinuity in the right femoral cortex anteriorly with slight impaction posteriorly (arrows), corresponding to a minimally displaced fracture of the greater trochanter. B: Coronal reformatted CT shows the extent of the fracture. On MRI, fracture lines are dark on T1-weighted images, with surrounding intermediate signal that may involve the adjacent marrow and soft tissues, corresponding to hemorrhage and edema (Fig. 1.13). On T2-weighted images, the surrounding edema and hemorrhage are high in signal intensity, while the fracture line remains dark. In compression fractures of cancellous bone, the fracture line may be absent, but the change in signal will be present if the fracture is acute. Avulsion fracture fragments may be difficult to identify on MRI, as the fragment itself may have the same dark signal on T1- and T2-weighted images as the soft tissue structure that pulled it off. Surrounding edema and hemorrhage should be present with acute fractures. Fractures caused by compressive loading tend to have greater amounts of adjacent marrow edema than fractures caused by tensile loading. FIGURE 1.13. Minimally displaced lateral tibial plateau fracture. A: Coronal T1-weighted MRI shows dark fracture line (arrow) with surrounding edema. B: Coronal inversion recovery MRI shows dark fracture line (arrow) with surrounding edema. On radionuclide bone scans, fractures are evident as regions of focal accumulation of radioactivity. However, because the accumulation of the radioactive tracer depends on increased bone metabolism, radionuclide bone scans are useful only after the healing process has begun and are not used in imaging acute trauma. Similar to bone, the soft-tissue structures of the musculoskeletal system deform when loaded. In addition to recoverable or elastic deformation, the soft tissues may also sustain nonrecoverable or nonelastic deformation. Creep is continuous deformation under an applied load, and stress relaxation is the decrease in internal load over time at a constant deformation. These viscous effects vary with time and the rate of loading, and the structure does not instantaneously recover its original size and shape when the load is removed. When a soft-tissue structure is loaded rapidly, it deforms elastically and perhaps fails if the load is great enough; if the same load is applied more slowly, creep and stress relaxation allow the structure to deform to a greater extent, permitting it to absorb more energy without failing. For these reasons, ligaments and tendons are stronger under tensile loading when the load is applied slowly rather than rapidly. Where they attach to bone, it is generally the rate of loading and the strength of the soft tissues relative to the bone that determine whether a soft-tissue or a bony injury is sustained. In general, rapid rates of loading cause the soft tissues to fail, whereas slower rates of loading avulse the bone. Injuries of tendons or muscle-tendon units are called strains; injuries of ligaments are called sprains. Injuries of either may also be called tears. Strains and sprains are classified by severity, with grade 1 being a mild injury and grade 3 being a severe, complete discontinuity (Table 1.1). Injuries to soft tissue alone without associated fractures are common and may be difficult to detect on radiographs. Soft-tissue injuries may be directly imaged by MRI and sonography. TABLE 1.1 Grading of Sprains and Strains
Approach to Trauma

 EPIDEMIOLOGY
EPIDEMIOLOGY
 BONE BIOMECHANICS
BONE BIOMECHANICS
Force And Deformation
Loading And Fractures







Bone Bruises

 IMAGING FRACTURES
IMAGING FRACTURES


 SOFT-TISSUE BIOMECHANICS
SOFT-TISSUE BIOMECHANICS
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


