– Extrapancreatic organ involvement common (∼ 60%); inflammatory bowel disease in only 2-6%
– Older patients (usually > age 60) with M > F
Type II: Idiopathic duct-centric pancreatitis
– No IgG4 tissue staining; serum IgG4 not elevated
– No extrapancreatic organ involvement; inflammatory bowel disease in 30%
– Younger patients (mean age 43) with M=F
(Left) Axial CECT shows diffuse infiltration and enlargement of the pancreas with loss of normal fatty lobulation. There is a hypodense halo or capsule around the pancreas, with relatively little spread into adjacent tissues, compatible with autoimmune pancreatitis. All symptoms and signs resolved with steroid therapy.
(Right) Transhepatic cholangiogram in a patient with autoimmune pancreatitis shows multifocal strictures indistinguishable from those of primary sclerosing cholangitis.
(Left) Axial CECT demonstrates a diffusely enlarged pancreas with a low attenuation halo around its margin.
(Right) Coronal CECT from the same patient shows similar findings with a low attenuation capsule around the enlarged pancreatic margin. Note the presence of biliary dilatation in this patient with a history of biliary strictures, often associated with autoimmune pancreatitis.




 MRCP: Multiple discontiguous MPD/bile duct strictures which resolve after secretin (duct penetrating sign)
MRCP: Multiple discontiguous MPD/bile duct strictures which resolve after secretin (duct penetrating sign)



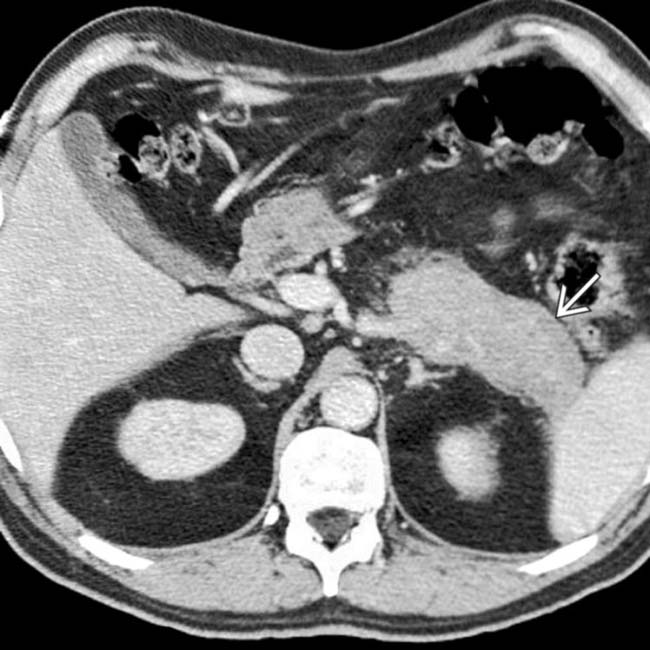
 around the pancreas, with relatively little spread into adjacent tissues, compatible with autoimmune pancreatitis. All symptoms and signs resolved with steroid therapy.
around the pancreas, with relatively little spread into adjacent tissues, compatible with autoimmune pancreatitis. All symptoms and signs resolved with steroid therapy.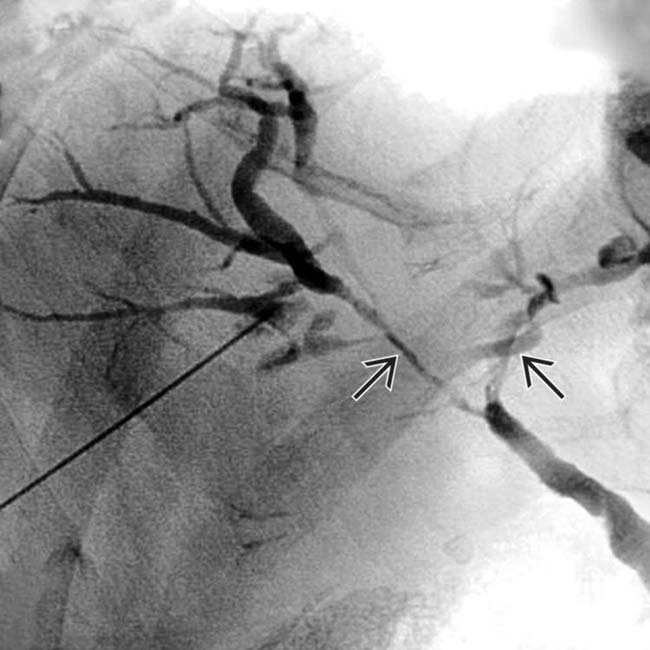
 indistinguishable from those of primary sclerosing cholangitis.
indistinguishable from those of primary sclerosing cholangitis.
 around its margin.
around its margin.
 around the enlarged pancreatic margin. Note the presence of biliary dilatation
around the enlarged pancreatic margin. Note the presence of biliary dilatation  in this patient with a history of biliary strictures, often associated with autoimmune pancreatitis.
in this patient with a history of biliary strictures, often associated with autoimmune pancreatitis.





 Diffuse sausage-like enlargement of pancreas (with smooth contour) and loss of pancreatic lobulations
Diffuse sausage-like enlargement of pancreas (with smooth contour) and loss of pancreatic lobulations Often less enhancement than expected in arterial phase; delayed enhancement of involved parenchyma/capsule
Often less enhancement than expected in arterial phase; delayed enhancement of involved parenchyma/capsule


















