Fig. 4.1
Example of a block design silent word generation paradigm: the paradigm begins with a 30 s resting (or control) block during which the patient is asked to simply stare at abstract symbols. The following 30 s the patient is engaged in a speech production task consisting of covertly generate words beginning with the presented letter. The resting and the active block are presented in alternating fashion every 30 s for 3–4 min. The subtraction of a visual fixation task from the language active task aims to eliminate visual activation from the expressive language activation maps
The fMRI literature distinguishes two general categories of paradigms: block design and event-related. In the block design method, the active and control tasks are presented in regular alternating epochs (blocks) and are usually labeled “on” (active) and “off” (control). The regions of the brain where there are statistically significant differences between the signal acquired during the on and off periods are considered as functionally active.
Event-related paradigms are designed presenting a single event at a time instead of epochs of multiple serial stimuli. Each event is considered separately as being time-locked to the beginning of the stimulus, and signal changes are explored in relation to the onset of the event generated by the trial.
After the image acquisition several preprocessing steps are needed before the statistical analysis that provides the activation maps can be performed. First, a four-dimensional dataset is created from the thousands of raw images where the signal time series recorded over the entire time of acquisition is reconstructed in each voxel (Fig. 4.2).
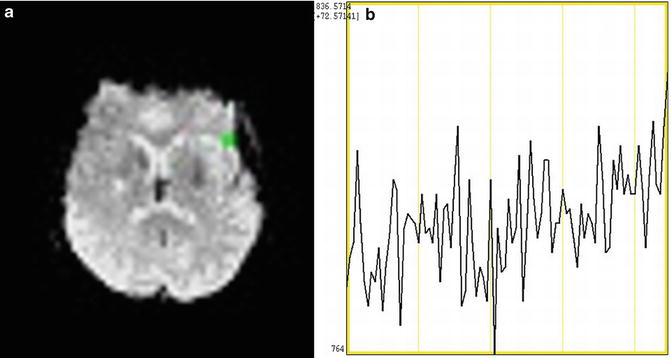
Fig. 4.2
(a) (Left) One BOLD EPI image (axial slice) as acquired and reconstructed from the scanner. In image (b) the time course of the signal in the voxel highlighted in green in (a) is reconstructed. Data have been processed utilizing the Analysis of Functional NeuroImages (AFNI) software package (afni.nimh.nih.gov)
Then for each volume all the slices are temporally shifted so that they were acquired at the same time and all the volumes are registered to a reference one to correct for minor head motion. Two further preprocessing steps, not necessarily performed in all analyses, are image spatial smoothing to enhance the signal to noise ratio (SNR) and spatial normalization to a common stereotactic space for neuroanatomical labeling.
After the preprocessing, several statistical methods can be used to infer neuronal activation.
The most commonly used method is the General Linear Model (GLM) that consists of a regression analysis where the paradigm timing is convolved with an expected hemodynamic response function (HRF), and the obtained waveform (the GLM) is fitted to the acquired time series voxelwise. A map of regressors is thus obtained in each voxel with an associated statistical significance (t-value, Z-score, or p-value). These maps are thresholded at an arbitrary significance level and suprathreshold voxels are overlaid as bright clusters on anatomical images, thus forming the so-called activation maps (Fig. 4.3).
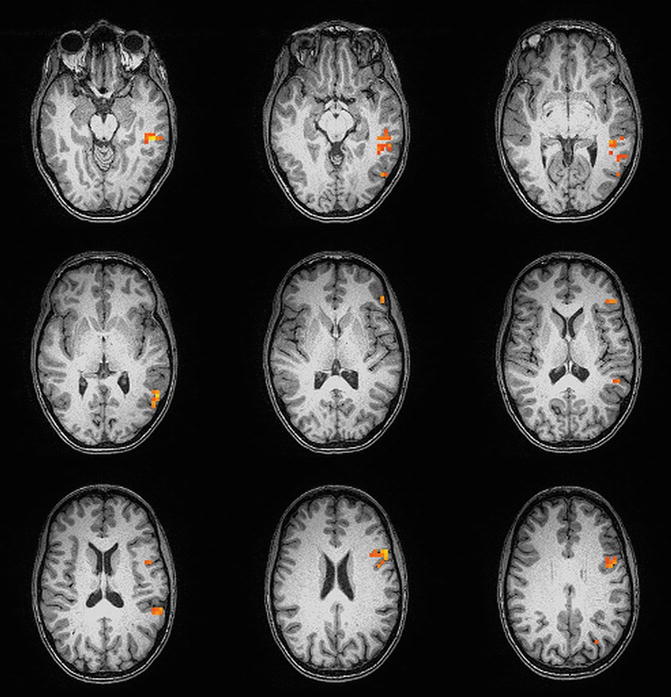
Fig. 4.3
Activation map in a right-handed normal volunteer from a sentence completion paradigm overlaid on T1 MPRAGE structural images. The bright spot pixels are the ones whose signal time series in the T2* EPI images demonstrates a statistically significant signal increase (thresholded at a t-value of 4.0, p < 0.0001) corresponding to performance of the language task compared to the baseline simple fixation task. The activation is mainly localized in the left (language dominant) cerebral hemisphere
The GLM data analysis approach is the most commonly used and widely accepted method, especially in the field of clinical fMRI, because it provides activation in expected areas and with anticipated timings [3]. In the last decade several exploratory and data driven techniques (e.g., Principal Component Analysis and Independent Component Analysis) have been developed that can be used to discover brain activity without the need to make a priori assumptions regarding areas of activation or timing of the HRF [4].
Clinical fMRI
BOLD fMRI has been used in neuroscience research studies to assess a broad spectrum of brain function. Since the early 1990s when this technique was first established, investigators have progressed from the study of basic motor and visual function to the investigation of more and more complex cognitive function, including language, memory, emotion, and even abstract reasoning functions utilizing fMRI. In the last decade BOLD fMRI has evolved from a purely research imaging technique to a viable clinical technique that is mainly applied for presurgical planning in patients with brain tumors and other resectable brain lesions. However the clinical use of fMRI for presurgical planning is limited today to the detection of sensorimotor, language/speech, and vision function, with currently only limited capability for accurate assessment of memory function. The standardization of the paradigms in terms of task performed, timing parameters, and postprocessing is still an evolving process, although many language and motor activation paradigms have been reported to provide results that are concordant with those obtained using “gold-standard” electrophysiologic intraoperative mapping techniques and are currently used in many institutions [5–10].
Two Current Procedural Terminology (CPT) codes were established in January 2007 as a result of numerous single-center clinical validation studies and several landmark studies that have demonstrated the clinical impact of preoperative functional imaging on surgical planning [11, 12].
The American Society of Functional Neuroradiology (ASFNR) has been established in 2004 with the aims to promote the introduction of BOLD fMRI and other functional neuroimaging techniques, such as Diffusion Tensor Imaging (DTI) or MR spectroscopic imaging (MRSI) and MR perfusion imaging into clinical neuroradiology practice and to develop standards for their practice, including the definition of protocols for image acquisition, processing, and quality control. This last issue can be very critical in clinical fMRI because BOLD data can be degraded by artifacts of different types that in turn can affect the reliability of the activation maps. Some of these artifacts, such as minor head motion and physiological noise, are imaging session-related and can be monitored during the scan and corrected by using dedicated algorithms in postprocessing. However, when the intravoxel signal change due to gross head motion is greater than the expected BOLD effect signal change, realignment algorithms can fail. 2 mm of translational head motion in any direction and 2° of head rotation about any axis are currently considered to be the thresholds above which a motion-degraded free reconstruction of the voxel signal time series cannot be guaranteed. Most of the vendors today are able to provide devices for monitoring cardiac pulsation and/or respiratory rate as well as software to assess head motion in real time.
Other sources of artifacts might be due instead to the patient’s conditions and clinical history. For example, the presence of blood products or surgical hardware in patients with previous surgery produces susceptibility artifacts that are accentuated in the BOLD fMRI images, because the sequences routinely used for fMRI are very sensitive to local magnetic field inhomogeneities. Decrease in the volume of activation in eloquent cortex adjacent to tumor has been reported that has been attributed to susceptibility artifacts [13].
Including a susceptibility-weighted imaging sequence in a fMRI protocol for presurgical planning can be helpful to determine regions of the brain where hemosiderin deposition or micromineralization exist. This is important for two reasons: (1) it helps characterize brain tumors or vascular malformations, and (2) it helps in quality control analysis of BOLD data by alerting the interpreting neuroradiologist to the possibility of false-negative activation due to excessive susceptibility artifact, which can severely impair ability to detect regional BOLD activation on GRE echoplanar images, which are particularly prone to susceptibility-related distortion.
Neurovascular uncoupling (NVU) is a further condition that could impair the detection of activation within or in spatial proximity to a brain structural lesion. As reported in the introduction of this chapter fMRI indirectly reveals neuronal activation through the detection of the increase in blood flow, volume, and oxygenation in the vessels and the parenchyma near the site of activation. However, many brain diseases (e.g., tumor, strokes, vascular malformation) are characterized by vasculature that reacts less vigorously than normal vessels to physiological stimuli. Therefore, in such conditions the BOLD signal change expected in a region of the brain activated by a particular stimulus can not be detected despite the possible presence of eloquent cortex. BOLD activation maps in these cases can be affected by type II errors (false negatives) and can misguide the neurosurgeons in the preoperative assessment of functional areas at risk of being resected during lesion resection.
Hypervascularized lesions, such as high grade gliomas or AVM, are expected to be affected by NVU because of their aberrant neovasculature [14]. In these cases regions of increased cerebral blood volume and blood flow that can be detected by MR perfusion imaging suggest the risk of NVU, and so caution should be used in the interpretation of the fMRI data in those regions.
However, cases of decreased CVR have been reported in low-grade gliomas [15], which generally do not show hyperperfusion or enhancement in postcontrast MR images. These results have been attributed to the infiltrative nature of glial tumors that compromises the neuronal contacts with the surrounding microvasculature and astrocytes, thus contributing to the attenuation of the BOLD effect.
Mapping the cerebrovascular reactivity (CVR) throughout the brain can provide a direct means of detection of NVU. CVR maps can be obtained by using a BOLD sequence itself while temporarily altering the PCO2 level in the brain microvasculature through a hypercapnia task. Since increase in PCO2 causes the dilation of cerebral blood vessels, without increasing the metabolic rate of brain parenchyma, and changes the deoxyhemoglobin (dHb) concentration in the cerebral vasculature, BOLD MR imaging can be used to test vascular reactivity following a hypercapnia challenge [16].
A breath-hold (BH) task and controlled CO2 inhalation are the most commonly utilized techniques to estimate CVR in humans. A BH task does not provide any quantitative measurement of CVR; however, such a task can be easily performed and included in a clinical fMRI protocol. A CO2 inhalation task can directly measure CVR by recording the change in end-tidal CO2, but it requires special equipment and dedicated personnel to be performed, and thus it is more difficult to routinely implement in a standard clinical setting.
BOLD fMRI Language Mapping for Presurgical Planning
The main goal of fMRI language mapping for presurgical planning is to provide neurosurgeons with two key bits of information: cerebral hemispheric language lateralization (dominance) and the spatial proximity of eloquent language cortical regions to potentially resectable brain lesions such as brain tumors. For this reason the paradigms designed for language mapping should elicit activation in the speech productive areas in the frontal lobe as well as the receptive language areas in the temporal and parietal lobes. The activation patterns provided by these paradigms should be limited to or predominantly involving the dominant language hemisphere, although degree of activation of contralateral hemispheric homologous regions on tasks that have been demonstrated to effectively lateralize language function is also important for surgical planning purposes. If cortical functional reorganization has occurred as a response of the brain to neoplastic infiltration of expected critical language areas, the neurosurgeon would benefit by fMRI’s capability of eliciting activation in these supplementary regions that may have been recruited as an adaptive response for preservation of overall language function. The language fMRI literature reports a large variety of different paradigms that have been used both in normal subjects and in patients. In clinical fMRI block design paradigms are usually the preferred choice because they are generally easier for most patients to perform and generally produce more statistically robust results. Although event-related paradigms better reflect the hemodynamic response and are not affected by the stimulus predictability as for block design paradigms, they require longer acquisition times and have lower statistical power.
They are usually categorized into three groups: expressive, receptive, and semantic paradigms. In the following subsections the paradigms most commonly used in clinical fMRI for each category are described. The choice of the paradigms that are administered depends mainly on the location of the lesion and the patient’s neurological deficits. For example if a tumor is located in the frontal lobe but does not suffer from a dense Broca’s aphasia that would preclude performance of such tasks, one or more expressive paradigms should be run to localize the functional Broca’s area and determine its distance from the margins of the lesion (Fig. 4.4). It is critical also to assess before the scan that the patient is not sufficiently cognitively impaired to perform a task or if such a task needs to be adapted in order to be performed by the patient; for example, the stimulus duration or frequency may need to be adjusted to account for the patient’s degree of cognitive decline or slowing. A training session should be carried out by presenting the patients with stimuli that are similar to the real test stimuli and asking them to perform the paradigm. During such a session, response accuracy and latency can be assessed in order to tailor the actual paradigm that the patient performs in the scanner to the individual patient’s needs and decide whether or not such a paradigm would be appropriate for such a patient.
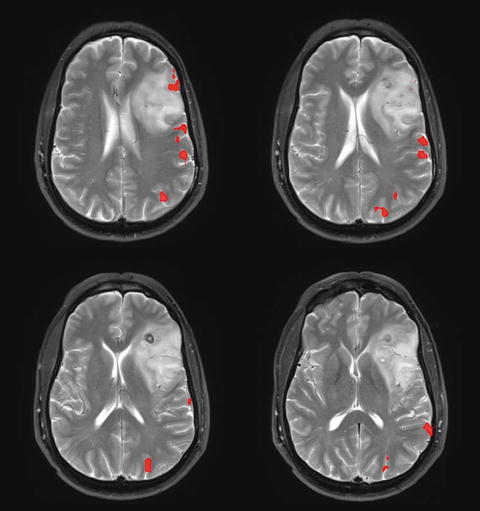
Fig. 4.4
Activation map in a patient with a left frontal lobe tumor obtained from performance of a silent word generation paradigm fused with T2 FLAIR structural images. Areas of neuronal activation are present both at the anterior and posterior margins of the lesion
Expressive Paradigms
Expressive paradigms are conceived and designed to elicit activation mainly in the speech production areas. Silent Word Generation, Silent Verb Generation, and Simple Object Naming are among the most used and cited verbal fluency paradigms in fMRI for presurgical mapping [17–19]. The block duration varies between 20 and 30 s and at MRI field strengths of 3 T or higher, three or four cycles of alternating control and active blocks are sufficient to provide enough statistical power for generation of robust activation maps.
In performing a silent word generation task, patients are asked to covertly generate words beginning with a presented letter during the active block, whereas for the silent verb generation task patients are asked to covertly generate verbs associated with a presented letter or word. The control block consists in both paradigms of a simple fixation task in order to exclude the visual component from the activation maps. The stimuli for the active tasks also can be delivered aurally, and in that case the control block consists of listening to computer-generated noise or other auditory stimulus devoid of linguistic content. The pattern of activation is equivalent for these two tasks and includes the dorsolateral prefrontal cortex (DLPFC), inferior frontal gyrus (IFG), variably within cingulate language regions, supplementary motor area (SMA), premotor and motor regions and occasionally the parietal, temporal, and/or occipital cortex depending on whether auditory or visual stimuli are used. These two tasks provide robust expressive language cortical activation and effective hemispheric language lateralization, especially of frontal regions. The main disadvantage, however, is that the patient’s performance cannot be objectively monitored but only assumed from patient’s evaluation during a training session performed outside the scanner and patient feedback provided to the technologist immediately after completion of one of these paradigms.
During the active block of simple object naming, patients are shown an object for 2 or 3 s and asked to silently name the presented object. Again a simple fixation task makes the control block. For this paradigm robust activation is provided in the IFG (frontal operculum), DLPFC, or premotor cortex, SMA, ventral occipito-temporal cortex (VOTC), and to a variable extent within the posterior temporo-parietal language cortex. Inferior temporal gyrus (ITG) activation is also seen commonly. It is not possible to monitor the patient’s performance in this task either, and in general the expected activation pattern does not allow as effective hemispheric language lateralization as with the silent word generation and silent verb generation tasks. However, this task is generally easy for most patients to perform, even those with cognitive impairment and in the pediatric population, and behaviorally it resembles confrontation naming tasks that are often performed in the operating room environment during awake intraoperative cortical stimulation mapping procedures.
The rhyming task, on the other hand, is an example of a phonological processing language paradigm, and as such may be categorized as an expressive language task. As implemented in most institutions, this is an example of a dual choice task, in which the patient’s responses can be easily monitored. During the active block of this paradigm, pairs of words are presented every 3 or 5 s and patients are required to decide whether the word pairs rhyme or not, and are asked to press a button on a keypad in cases of affirmative responses only (Fig. 4.5b). In the control block, as implemented in our institution, two rows of stick figures are presented at the same stimulus presentation rate as the pairs of words presented in the active blocks, and patients have to judge whether the two rows exactly match or not; they are asked to press a button on a keypad in cases of affirmative responses (Fig. 4.5a).
Fig. 4.5
Example of visual stimuli for a phonological (rhyming) paradigm. During the control block the patient is asked to judge whether two rows of stick figures exactly match or not (see an example in (a)), whereas during the active block he is asked to judge whether pairs of words rhyme or not (see an example in (b)). The patient’s response is monitored and recorded through a button press on a keypad
Another version of the control block that we have used can be designed where patients are shown nonsense line drawings with a + sign in one of the lower corners of the slide. In this alternate version of the rhyming task, the subjects are instructed to press a button on the left side of keypad if the + sign is in the left corner or a button on the right if the sign is in the right corner [20].
Activation is identified in the DLPFC, IFG, and superior temporal gyrus (STG) and cortex lining the superior temporal sulcus (STS); the VOTC also demonstrates activation, typically in a left hemispheric dominant fashion corresponding to the visual word area. DLPFC and premotor/SMA activity is minimized by the control condition. Rhyming can be a challenging task for some patients to perform because of the demanding nature of the control task and role of the arcuate fasciculus in phonological processing; however, it is a very promising and effective lateralizing task and shows an activation pattern that is clearly more language-specific than that of the silent word generation task [21].
Receptive Paradigms
These paradigms are designed to identify mainly receptive language regions in the temporal and parietal lobe, such as the Wernicke’s area (the posterior aspect of the left STG) and, in some cases, its right hemispheric homologue. The typical active block involves a language (reading or listening) comprehension task for 20 or 30 s alternating with a control block that in general is designed to activate all but the language areas involved in performing the active language comprehension task. The GLM analysis that looks for statistically significant difference in the signal between the control and the active block detects activation only in voxels located in specific language areas. Sentence reading or listening comprehension is a typical example of a receptive language paradigm [22]. During the active block patients are asked to read or listen to a series of sentences and decide whether each of these individually presented sentences is true or false. Patient performance is monitored by a button press response that is required in cases in which the presented sentence is true. The control block, as designed at our institution, consists of a string of nonsense symbols without any linguistic content, which the patient is asked to visually scan as if reading (serving as a control for visual processing and orthographic language processing) for the sentence reading comprehension task. Similarly, for the sentence listening comprehension task, the patient is asked to press the button on the keypad for true sentences (and not for false sentences) that are presented as auditory stimuli in the active block, but they are asked to refrain from button pressing during the control block, when they simply listen to nonsense sounds without linguistic content.
These two paradigms are not found to be effective for determining patient hemispheric language dominance, but their activation maps, when combined with the ones obtained through the use of more effectively lateralizing tasks often yield a comprehensive representation of the entire language network (Fig. 4.6) including Broca’s area (BA, left IFG), Wernicke’s area (WA, posterior left STG), and their right hemispheric homologues, DLPFC, ITG, middle temporal gyrus (MTG), angular (AG) and supramarginal gyrus (SMG), other parietal language cortices and SMA.
Get Clinical Tree app for offline access
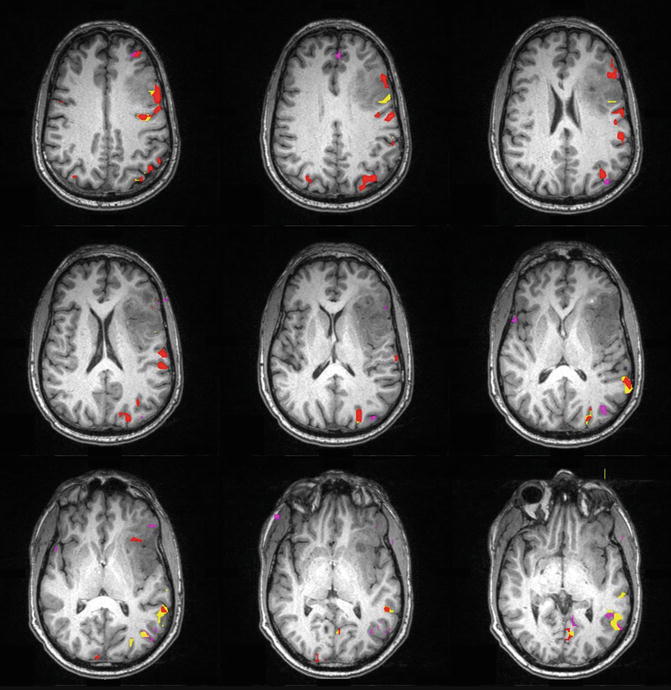
Fig. 4.6
Composite language activation map from silent word generation (color-coded as red), sentence completion (yellow), and listening comprehension tasks (magenta) in a patient presenting with a lesion in the left frontal lobe involving the frontal operculum with extension to the insular cortex and subinsular white matter. The statistical threshold was set to 0.35 cross correlation for each paradigm with three voxel clustering (spatial extent) threshold also applied. The combination of the activation from these three paradigms includes most of the typical language representation areas in the left (dominant hemisphere), including Wernicke’s area (WA), located in the left superior temporal gyrus (STG) and Broca’s area (BA) in the left inferior frontal gyrus (LIFG) as well as dorsolateral prefrontal cortex (DLPFC) and language (or pre-) SMA (supplementary motor area)
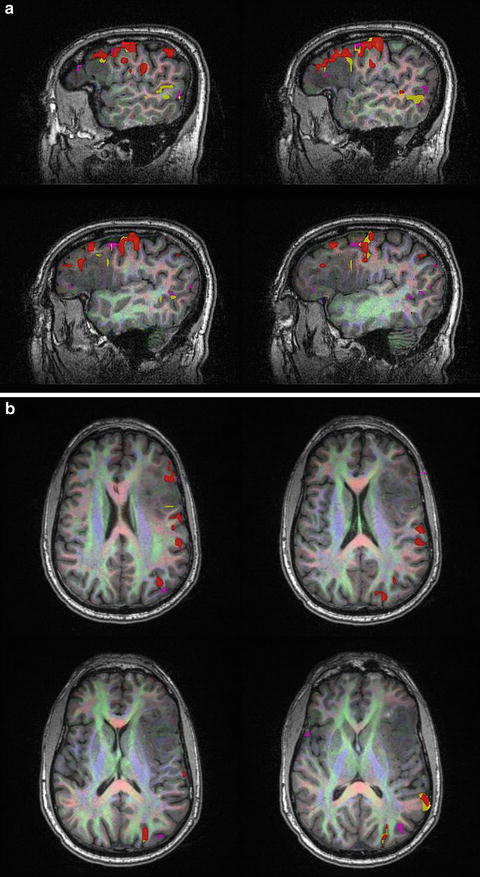
Fig. 4.7
(a) Composite language activation map from a silent word generation (coded as red), sentence completion (yellow), and listening comprehension task (magenta) in the same patient as in Fig. 4.6, but superimposed on fractional anisotropy (FA)-weighted color directional diffusion maps that have been overlaid on 3D MPRAGE (magnetization-prepared rapid acquisition gradient echo) anatomic images. These maps follow the standard RGB convention, whereby red refers to preferential medial-lateral diffusion, green
 Imaging Metabolic and Molecular Functions in Brain Tumors with Positron Emission Tomography (PET)
Imaging Metabolic and Molecular Functions in Brain Tumors with Positron Emission Tomography (PET)
 BOLD fMRI for Presurgical Planning: Part II
BOLD fMRI for Presurgical Planning: Part II
 Role of Amide Proton Transfer (APT)-MRI of Endogenous Proteins and Peptides in Brain Tumor Imaging
Role of Amide Proton Transfer (APT)-MRI of Endogenous Proteins and Peptides in Brain Tumor Imaging
 Diffusion Tensor Imaging: Introduction and Applications to Brain Tumor Characterization
Diffusion Tensor Imaging: Introduction and Applications to Brain Tumor Characterization
 Proton Magnetic Resonance Spectroscopy and Spectroscopic Imaging of Primary Brain Tumors
Proton Magnetic Resonance Spectroscopy and Spectroscopic Imaging of Primary Brain Tumors
 Ultra-High Field MRSI (7T and Beyond)
Ultra-High Field MRSI (7T and Beyond)




Related posts:
Imaging Metabolic and Molecular Functions in Brain Tumors with Positron Emission Tomography (PET)
BOLD fMRI for Presurgical Planning: Part II
Role of Amide Proton Transfer (APT)-MRI of Endogenous Proteins and Peptides in Brain Tumor Imaging
Diffusion Tensor Imaging: Introduction and Applications to Brain Tumor Characterization
Proton Magnetic Resonance Spectroscopy and Spectroscopic Imaging of Primary Brain Tumors
Ultra-High Field MRSI (7T and Beyond)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
