Bone marrow edema (BME) is a frequent but nonspecific imaging finding encountered in a wide range of musculoskeletal disorders, including fractures, infection, inflammatory arthritis, and neoplasia. While MR imaging is considered the reference standard for detection of BME, dual-energy computed tomography (DECT) offers a valuable alternative, particularly in emergent settings or when MR imaging is contraindicated. This article outlines the principles and acquisition strategies of DECT, including dual-source, rapid kilovoltage peak switching, and dual-layer spectral detector techniques. Integration of DECT into clinical workflows can enhance diagnostic accuracy, especially in acute care and resource-limited settings.
Key points
-
•
DECT enables rapid, accurate detection of bone marrow edema and assists in evaluating musculoskeletal disorders, including fractures, arthritis, osteomyelitis, and neoplasms.
-
•
Virtual noncalcium DECT enhances bone marrow edema detection by removing calcium, improving visualization of marrow infiltration and aiding early diagnosis and treatment assessment.
-
•
DECT effectively detects BME, but radiologists should watch for pitfalls such as false positives from sclerosis, red marrow hyperplasia, and skin artifacts.
-
•
Integrating DECT into clinical workflows improves diagnostic accuracy and efficiency, especially when MRI is unavailable or impractical, such as in emergency settings.
Abbreviations
| AVN | avascular necrosis |
| BME | bone marrow edema |
| CI | confidence interval |
| CT | computed tomography |
| DECT | dual-energy computed tomography |
| HAP | Hydroxyapatite |
| MSU | monosodium urate |
| OCLs | osteochondral lesions |
| PCCT | photon-counting CT |
| RA | rheumatoid arthritis |
| SF | stress fracture |
| SR | stress reaction |
| VCFs | vertebral compression fractures |
| VNCa | virtual noncalcium |
Introduction
Bone marrow edema (BME) is characterized by an abnormal accumulation of fluid within the bone marrow and is commonly associated with a variety of musculoskeletal pathologies. Accumulation of fluid and blood products in the marrow space secondary to trabecular microfractures and associated capillary disruption is a recognized mechanism of BME. Elevated levels of bone-specific alkaline phosphatase, procollagen type 1 N-terminal propeptide, and angiogenic factors are often observed in histologic samples obtained from areas of BME, reflecting the active bone turnover and reparative response. BME can result from both traumatic and nontraumatic etiologies, including infectious, inflammatory, and neoplastic causes. In osteomyelitis, capillary leak, increased vascularity, and inflammation contribute to BME, while in neoplastic lesions, increased vascular permeability and vascularity may similarly manifest as BME. Early detection of BME is essential for effective management and prevention of further complications. However, BME can be missed in the early stages on conventional imaging modalities such as computed tomography (CT). Although conventional CT effectively visualizes bone structure and fractures, it is not sensitive for detecting BME.
MR imaging is the gold standard for assessing BME and provides superior visualization of soft tissues, making it an invaluable tool in the diagnosis of limb injuries. , However, it has several limitations, including higher cost, longer scan times, and limited availability in emergency settings. Dual-energy CT (DECT) provides the advantages of rapid scanning and enhanced detection of subtle edema, particularly in acute settings. By utilizing 2 different x-ray energy levels, DECT enables differentiation of tissues based on atomic composition, allowing the detection of BME and adjacent bone structures with high accuracy. ,, Diagnostic performance of DECT in detecting BME in lower limb joint injuries revealed sensitivity of 0.82 (95% confidence interval [CI]: 0.76 to 0.87) and specificity of 0.95 (95% CI: 0.92–0.97).
This article discusses the clinical applications of DECT in the detection of BME, outlines its diagnostic performance, and highlights its advantages over conventional imaging modalities. Additionally, it emphasizes the importance for radiologists to recognize the various pathologies that present with BME to help with providing accurate differential diagnosis. Potential pitfalls and interpretative challenges are also reviewed to ensure optimal utilization of DECT in clinical practice.
Dual-energy computed tomography principles and techniques
In conventional CT, a single x-ray beam with a fixed energy level acquires images of the body. However, this approach may limit the ability to differentiate tissues with similar attenuation properties. DECT overcomes this limitation by acquiring images at 2 distinct energy levels, typically 80 and 140 kVp, as different materials exhibit unique attenuation at varying photon energies. This enables material characterization based on atomic number and electron density. For instance, substances with low atomic numbers, such as water, exhibit minimal attenuation variation across energy levels, whereas high atomic number materials, such as iodine, show significant differences.
DECT can be implemented through several methods: (1) dual-source systems, which employ 2 x-ray tubes and detectors operating at different energies and positioned at different angles, allowing simultaneous acquisition of low-energy and high-energy datasets; (2) rapid kilovoltage peak switching, where a single x-ray tube alternates between low-energy and high-energy levels during a single gantry rotation, but may be limited by tube heating and cooling constraints; (3) dual-layer spectral detectors, which utilize a specialized detector with 2 layers, the upper layer absorbing low-energy photons and the lower capturing high-energy photons; and (4) split-filter techniques, which use predetector filters to divide a single x-ray beam into 2 distinct energy spectra. Each approach offers specific advantages in terms of spectral separation, temporal resolution, and radiation dose efficiency.
Another advantage of DECT is artifact reduction, particularly in the context of metallic prostheses. Beam hardening artifacts result from attenuation of low-energy photons within a polychromatic x-ray beam contributing to radiation scattering. By generating virtual monoenergetic or composition-specific images, DECT removes these low-energy photons, reducing image noise and artifacts. This is clinically important when evaluation is limited by streak or beam-hardening artifacts, such as in patients with knee or hip prostheses.
Virtual Noncalcium Imaging
A commonly used 3 material decomposition algorithm enables the detection of fat, soft tissue, and bone mineral within each voxel. When bone mineral composed primarily of calcium is removed from the dataset, virtual noncalcium (VNCa) images can be generated. DECT can generate VNCa images by virtually removing calcium content from the CT dataset, resulting in “calcium-free” images. This allows for improved visualization of the bone marrow without interference from the surrounding bone, which is particularly useful in the detection of BME. , Additionally, color-coded overlay images can be produced and superimposed on the CT scan, highlighting regions of edema with enhanced clarity. In oncologic imaging, VNCa can facilitate the detection of bone marrow infiltration, enabling earlier diagnosis and assessment of treatment response. Two-material decomposition can be performed on DECT devices from any manufacturer, while 3 material decomposition such as VNCa requires specific postprocessing software, which is not available on all DECT devices.
Traumatic causes
Stress Fracture
Stress fracture (SF), including insufficiency and fatigue fracture, occurs due to excessive repetitive stress on healthy bone or from normal stress applied to weakened bone. It accounts for approximately 10% of all overuse sport injuries. Early diagnosis is critical to prevent progression to complete fracture and complications such as nonunion or delayed healing. The diagnosis of SF is typically based on the identification of a clear fracture line, while BME is considered a significant feature of stress reaction (SR).
MR imaging is the most sensitive imaging modality for detecting SF, SR, and associated BME. DECT can also detect BME in cases where a fracture line is not clearly visible, making it a valuable tool in patients with contraindications to MR imaging or in emergency settings where rapid assessment is required. MR imaging findings include the presence of a fracture line, BME, cortical thickening, and periosteal reaction. DECT also shows high specificity and good sensitivity for detecting SR and BME, particularly in cases without an identifiable fracture line. However, cortical bone thickening and sclerosis, common bone reactions in repetitive stress can reduce the sensitivity of DECT due to artifacts that interfere with the VNCa subtraction process. This limitation may hinder BME detection in certain cases.
DECT is particularly beneficial in young individuals, where the presence of red marrow and thick cortical bone may lead to false positives on conventional CT. In cases with subchondral sclerosis or previously healed fractures without a visible fracture line, the presence of BME may aid in diagnosis. DECT’s ability to delineate the extent of BME can be useful in evaluating treatment response and fracture healing. A meta-analysis of DECT sensitivity for BME detection was 0.80, 0.84, and 0.80 for knee, hip, and ankle joint injuries, respectively. The highest specificity was observed in hip injuries (0.97), which may be due to the anatomic and biomechanical characteristics of the hip joint, as its larger and more uniform bone structure facilitates more accurate detection and characterization. The accuracy of DECT in detecting BME may be reduced in stabilized (casted or splinted) and subacute extremity fractures, as both the frequency and area of BME are significantly lower compared to nonstabilized and acute fractures (416 vs 818 mm 2, P =.01), which can limit the diagnostic sensitivity of DECT in these cases.
Vertebral Compression Fracture
Single-energy CT of the spine is commonly used for the assessment of suspected vertebral compression fractures (VCFs). However, in cases of osteoporosis, minor fractures, old fractures with recurrent fractures, and occult fractures, single-energy CT may not be able to distinguish acute from chronic vertebral fractures. DECT is a promising tool for the detection of BME in acute vertebral fractures ( Figs. 1 and 2 ), yielding results comparable to MR imaging and superior to single-energy CT. Meta-analysis revealed that DECT had a pooled sensitivity of 89% (95% CI: 84%–92%) and specificity of 96% (95% CI: 92%–98%) for detecting vertebral body BME. There is a significant difference in water concentration on color-coded water-hydroxyapatite (HAP) images of DECT between acute and chronic VCFs, whereas there is no significant difference between chronic fractures and normal vertebrae.
Subacute vertebral compression fracture. A 76 year old female patient with back pain. Sagittal CT image ( A ) demonstrates lumbarization of S1. A compression fracture of the L1 vertebral body is observed without associated kyphosis, showing no significant decrease in vertebral body height. No surrounding fat stranding or hematoma is noted. Sagittal reconstructed dual-energy images ( B ), optimized for bone marrow depiction, reveal mild bone marrow edema along the fracture line ( arrow ), suggesting a subacute compression deformity of the L1 vertebral body.
Acute vertebral compression fractures. A 19 year old female patient presents with back pain following trauma. Double density in the superior endplates of the T7, T8, T10, and T11 vertebral bodies ( A ) suggests compression fractures. Dual-energy images ( B , C ) of the thoracolumbar spine show heterogeneous attenuation at the areas of wedging at T7, T10, and to a lesser degree at T8 and T11 (ovals), suggestive of bone marrow edema. The constellation of findings is consistent with acute anterior compression fractures at multiple levels.
In the setting of acute VCFs, hemorrhage, edema, and interstitial fluid and blood increase because of trabecular microfractures. Water-HAP imaging can be used to virtually subtract the HAP concentration, a major mineral component of bone, to display the water composition present in VCFs. The study demonstrated that DECT water-HAP and T2-weighted MR images are highly consistent in the setting of acute VCFs. When an acute VCF occurs, hemorrhage and BME appear as hyperintense signals on T2-weighted images, which is reflected by DECT water-HAP imaging. DECT water-HAP has been shown to have similar accuracy to MR imaging but offers the advantage of being a faster imaging modality for evaluating acute versus chronic VCFs, particularly in the emergency setting. False-positive results may occur in cases of Modic type 1 vertebral endplate changes, which appear similarly on MR imaging as hypointense on T1-weighted images and hyperintense on fluid-sensitive sequences. These changes resemble traumatic BME on water-HAP images.
Occult Fracture
Conventional radiography is the initial imaging modality for evaluating suspected hip or pelvic fractures. However, occult fractures may be present in approximately 3% to 10% of cases where radiographs initially appear normal. As occult fractures can lead to debilitating pain and significant morbidity, prompt diagnosis is critical, and additional imaging should be pursued when there is a high clinical concern. A delayed diagnosis may result in complications such as nonunion, fracture displacement, avascular necrosis (AVN), and the need for more extensive surgery that can increase patient mortality. With its ability to detect BME, DECT enhances the identification of occult fractures by revealing subtle trabecular or cortical disruptions that may be missed on conventional radiography or CT ( Figs. 3–5 ). DECT demonstrated 99% sensitivity and 100% specificity, with a significantly higher accuracy compared to radiographs and conventional CT in a retrospective study. Moreover, DECT can help identify intertrochanteric extension of femur fractures by demonstrating BME in this region, even in the absence of trabecular displacement in the presence of osteoporosis.
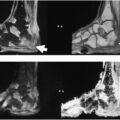
Bone contusion and fracture. A 21 year old male patient with knee trauma. Acute nondisplaced coronally oriented fracture ( arrows ) through the lateral femoral condyle ( A , B ), extending from the central weight-bearing articular surface cranially to the lateral femoral epicondyle, best appreciated on the sagittal image ( B ). Dual-energy virtual noncalcium color maps ( C ) also demonstrate a bone contusion involving the lateral tibial plateau in addition to lateral femoral condyle supporting trabecular injury and marrow contusion.
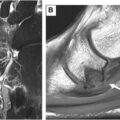
Acute femoral neck fracture. A 66 year old female patient presented with pain following a fall. Sagittal ( A ) and coronal ( B ) CT images demonstrate an obliquely oriented, minimally displaced acute transcervical femoral neck fracture. Dual-energy images ( C , D ) of the left hip confirm marrow edema at the fracture site.
Acute tibial fracture. A 23 year old male patient presents following knee trauma. Coronal ( A ) and sagittal ( B ) CT images show trabecular disruption with mild compression within the lateral tibial plateau, corresponding to areas of bone marrow edema on DECT images, consistent with a lateral tibial plateau fracture (Schatzker type 3) ( C , D ).
However, the accuracy of DECT is limited in the axial skeleton, particularly in deep areas such as the spine and pelvis, due to challenges with imaging complex bone structures and poor penetration of low-voltage beam. In contrast, DECT demonstrates superior sensitivity and accuracy in the extremities, particularly in more exposed joints and limb areas and tuberosities, where bone structures are less complex and artifacts are minimized. A study showed that DECT demonstrated a sensitivity of 100% and specificity of 99.5% in detecting occult fractures in patients with carpal fractures. Foti and colleagues used a third-generation DECT with VNC imaging on 40 consecutive patients. DECT values were significantly different between injured and noninjured (mean − 12.6 vs − 64.2, P <.001). DECT values showed a significant difference between injured and noninjured cases (mean −12.6 vs −64.2, P <.001). Using a −20 HU threshold to, the model achieved an AUC of 0.896, with sensitivity, specificity, and accuracy values of 88.0%, 92.6%, and 87.5%, respectively.
Pathologic Fracture
Pathologic fracture is defined as a fracture through weakened bone due to an underlying lesion, which may be a benign or malignant neoplasm, or osteomyelitis. Diagnosing pathologic fractures can be challenging for radiologists, and MR imaging is considered one of the most reliable imaging modalities to differentiate between pathologic and nonpathologic fractures. Several radiologic features aid in identifying pathologic fractures. In vertebral fractures, findings such as pedicle or posterior element involvement, paravertebral soft tissue thickening greater than 10 mm, absence of intradiscal gas, and cortical bone destruction suggest a neoplastic pathologic fracture. In long bones, the presence of a homogeneous lesion with well-defined margins is more indicative of a neoplastic process. Furthermore, hemorrhage and edema associated with acute traumatic fractures tend to appear more infiltrative on MR imaging. In the acute and emergency setting, DECT can assist in characterizing pathologic fractures by depicting BME patterns associated with neoplastic lesions, which differ from the linear BME patterns typical of traumatic fractures. Hemorrhage into the bone associated with traumatic fractures may sometimes mimic pathologic fractures on DECT; however, the absence of trabecular or cortical permeative-eroded margins and the presence of contiguous bone involvement can help distinguish traumatic from pathologic fractures. DECT can help distinguish between hematomas at acute traumatic fracture sites and neoplasms at pathologic fractures by detecting significantly different marrow Hounsfield unit values.
Nontraumatic causes
Osteomyelitis
Spondylodiscitis is an inflammation of the vertebral bodies and intervertebral discs. It can be classified based on the microorganisms involved, with pyogenic spondylodiscitis being the most common type. The condition typically begins in the intervertebral disc spaces and vertebral endplates, with subsequent involvement of the epidural space and paraspinal soft tissues. MR imaging is the best modality for diagnosing spondylodiscitis, as it typically shows disc edema, erosion of vertebral endplates, and paraspinal or epidural abscesses and inflammation. Foti and colleagues revealed that the overall sensitivity (0.91 vs 0.94), specificity (0.89 vs 0.93), and accuracy (0.90 vs 0.93) of DECT are lower than those of MR imaging; however, the observed differences between DECT and MR imaging are not statistically significant ( P >.05), suggesting that DECT could be a reliable tool for diagnosing spondylodiscitis. Endplate erosions exhibit the highest sensitivity on DECT, while the accuracy of BME is inferior to that of endplate erosions. The appearance of spondylodiscitis on CT depends on the stage of the disease. Endplate erosions usually indicate earlier stages, while sclerotic changes may indicate reparative changes and predict subsequent negative biopsy results. DECT could be a reliable imaging tool for diagnosing spondylodiscitis, with accuracy comparable to that of MR imaging. Given its rapid and cost-effective nature, DECT can be considered a suitable alternative to MR imaging.
In patients with diabetic foot syndrome, early diagnosis of pedal osteomyelitis is critical to prevent further complications and limit the spread of infection. Approximately 50% of diabetic patients with a foot ulcer develop adjacent bone osteomyelitis. MR imaging remains the standard-of-care imaging modality for evaluating suspected pedal osteomyelitis ( Fig. 6 ). However, in patients unable to undergo MR imaging, DECT with BME maps offers a valuable alternative, demonstrating a sensitivity of 77% and specificity of 86%. Notably, DECT with fat maps has shown superior diagnostic accuracy compared to BME maps, with sensitivities of 61% and 47%, respectively. DECT fat maps also correlate more strongly with bone marrow fat loss at T1-weighted MR imaging. Diagnostic performance improves further when VNCa images are combined with bone and soft tissue reconstructions.
( A , B ) Stump viability. A 72 year old male patient with a history of type 2 diabetes mellitus and congestive heart failure presents with a cold right foot and right calf vessel occlusion. He is being evaluated for infection following a below-knee amputation. DECT of the lower extremity with iodine contrast map reconstruction demonstrates a paucity of enhancement in the muscle at the distal stump (annotated area), consistent with ischemia, and bordering hyperemia in viable tissues. No rim-enhancing fluid collections are observed. There is no evidence of abnormal bone marrow edema or enhancement, confirming the absence of osteomyelitis.
Inflammatory Arthritis
Early pathologic changes of rheumatoid arthritis (RA) include tenosynovitis, synovitis, BME, and bone erosion. DECT is generally well tolerated in patients with joint pain and swelling and provides high-resolution evaluation of both bone and soft tissues, with a clear depiction of joint structures and their spatial relationships. DECT has demonstrated high sensitivity and specificity in detecting BME and can effectively facilitate the assessment of underlying soft-tissue abnormalities.
BME is a key indicator of active inflammation and plays a critical role in guiding therapy and follow-up in patients with RA. Color-coded DECT iodine maps help differentiate normal bone marrow from BME and correlate well with edema observed on MR imaging. On DECT, BME in RA is seen as regions of increased attenuation in the bone marrow adjacent to inflamed joints. This edema is often most pronounced near the areas of synovial inflammation and can be used to assess the degree of disease activity. DECT can also assess tenosynovitis, synovitis, and bone erosions in RA. Inflammatory lesions such as tenosynovitis and synovitis are essential findings in the early diagnosis of RA. Initiating biologic therapy in the early stages before destructive changes occur has been associated with improved outcomes. Recognition of subclinical inflammation detectable only by imaging has increased, indicating potential for further disease progression and predicting bone erosion.
A combination of high-resolution CT and iodine mapping may be used to evaluate early stage RA. Synovitis, defined as inflammation of the synovial lining of the joint capsule, occurs in various forms of arthritis, including inflammatory, infectious, and degenerative types. In RA, the synovium is the primary site of inflammation, and pannus formation is a hallmark of bone destruction. According to the Outcome Measures in Rheumatology Clinical Trials group, synovitis is defined as an area of synovial thickening and enhancement exceeding that of normal contrast-enhanced synovium, with a thickness greater than the width of the normal synovium. Fat-suppressed MR imaging sequences and short tau inversion recovery (STIR) images can effectively detect synovitis. Synovial proliferation (pannus) and inflamed synovium can also be visualized with DECT.
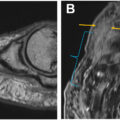
Tenosynovitis is defined as inflammation of the synovial lining of the tendon sheath. DECT with contrast enhancement demonstrates tenosynovitis as abnormal enhancement along the tendon, similar in appearance to contrast-enhanced MR imaging. Extensor peritendinitis at the metacarpophalangeal joints appears as inflammation surrounding tendons not enclosed by a synovial sheath, finding more characteristic of psoriatic arthritis (PsA) than RA. DECT can generate appropriate images to visualize extensor peritendinitis. Additional findings in PsA include extensor tendon enthesitis ( Fig. 7 ) and abnormal enhancement of the nail bed, which are in proximity and may reflect continuous inflammation. These changes typically affect the peripheral aspect of the fingers. DECT can also depict collateral ligament enthesitis and extra-articular enthesitis, which are important inflammatory lesions seen in PsA and other spondyloarthropathies.
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
 Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Evolving MR Imaging Applications in Posterior Tibial Tendon Dysfunction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


