Tumor location
Definition
GTV to CTV margin
CTV to PTV margin
Elective nodal coverage
Dose
Upper esophagus
Above carina
Primary: 3 ~ 5 cm longitudinally; 0.5 ~ 1 cm circumferentially
No IGRT: 0.5 ~ 1.0 cm
Periesophageal, mediastinal, supraclavicular
Neoadjuvant: 40 ~ 50.4 Gy in 1.8 ~ 2 Gy per fraction
Involved lymph node: 0.5 ~ 1 cm in all directions
IGRT: 0.5 cm
Definitive: 50.4 Gy (up to 66 Gy for tumor at cervical esophagus) in 1.8~2 Gy per fraction
Lower esophagus
Below carina
Same as upper esophagus
Same as upper esophagus
Periesophageal, mediastinal, perigastric, celiac
Neoadjuvant: 40~50.4 Gy in 1.8~2 Gy per fraction Definitive: 50.4 Gy in 1.8~2 Gy per fraction
In all esophageal malignancies, the entire esophagus from cricoid cartilage to EGJ and bilateral lungs should be contoured for proper DVH analysis. In upper esophagus tumors, the brachial plexus, larynx, and spinal cord should be contoured. In lower esophagus tumors, the heart, liver, stomach, duodenum, bilateral kidneys, and spinal cord should be delineated.
The gross tumor volume (GTV) consists of primary esophageal tumor (the greatest extension on CT, EUS, or FDG-PET) and involved lymph nodes. Lymph nodes with biopsy proof, increased FDG uptake, or enlarged short-axis diameter are delineated as GTV. The EUS can be used to better classify small paraesophageal lymph nodes that are difficult to classify on CT or FDG-PET scan.
Standard GTV to clinical target volume (CTV) expansions for the primary tumor are 3–5 cm in the longitudinal direction and 0.5–1 cm in the circumferential direction. The larger margins are applied in the longitudinal direction to account for submucosal spread (Gao et al. 2007). For involved lymph nodes, a 0.5–1-cm margin to all directions can be utilized. The CTV can be shaved off normal structures accordingly to respect anatomical boundaries. These margins can be adjusted based on the treating physician’s confidence about the disease extension (Figs.1, 2, and 3).

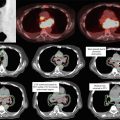
Fig. 1




Locally advanced (cT3N1M0) esophageal squamous cell carcinoma of middle esophagus with paraesophageal lymphadenopathy. The primary tumor was located at 25–32 cm below incisors. A representative FDG-PET image is shown to facilitate GTV (in red) contouring. 4-cm longitudinal and 0.5- to 1-cm circumferential margins were added for the CTV (in green) of the primary tumor. The bilateral supraclavicular lymphatics were covered electively in the presence of upper paraesophageal lymph node metastasis
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
