, Chia-Chun Wang2, Inigo San Miguel3 and Laura A. Dawson3
(1)
Graduate Institute of Oncology, National Taiwan University College of Medicine, Taipei, Taiwan
(2)
Division of Radiation Oncology, Department of Oncology, National Taiwan University Hospital, Taipei, Taiwan
(3)
Department of Radiation Oncology, Princess Margaret Cancer Centre, University of Toronto, Toronto, ON, Canada
Abstract
Three-dimensional conformal radiation therapy (3DCRT) has been the standard technique for hepatocellular carcinoma (HCC). Intensity-modulated radiation therapy (IMRT) may be useful to improve target coverage and for normal organ sparing, especially in the setting of unusually shaped target volumes. More recently, stereotactic body radiation therapy (SBRT) has been increasingly used. Individualized prescription doses are commonly used due to variable liver volume irradiation and proximity to luminal gastrointestinal tissues.
1 Hepatocellular Carcinoma
1.1 General Principles of Planning and Target Delineation
Three-dimensional conformal radiation therapy (3DCRT) has been the standard technique for hepatocellular carcinoma (HCC). Intensity-modulated radiation therapy (IMRT) may be useful to improve target coverage and for normal organ sparing, especially in the setting of unusually shaped target volumes. More recently, stereotactic body radiation therapy (SBRT) has been increasingly used. Individualized prescription doses are commonly used due to variable liver volume irradiation and proximity to luminal gastrointestinal tissues.
In addition to a history and physical exam, laboratory examinations, a liver function assessment, and imaging studies should be obtained for diagnosis, staging, and planning. Patients should undergo a contrast-enhanced (preferably triphasic [arterial, portal-venous, and delayed phases]) computed tomography (CT) scan of the liver, with 3–5 mm slice thickness. Multiphase dynamic magnetic resonance imaging (MRI) scans can be used if CT contrast is contraindicated. Additionally, MRI scans may be complimentary to CT scans for target delineation. 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET) images may be helpful in localizing the viable tumor(s) of individual cases such as patients with recurrent tumor(s) at previous lipiodol retention and/or radiofrequency ablation areas.
Half-body or whole-body immobilization with respiratory control is needed for better reproducibility. Devices such as a vacuum bag or chest board may be used to immobilize a patient, preferably with arms up, during simulation and used throughout the course of treatment. This will enable reproducibility and allow spatial freedom of beam directions. The systems for respiratory coordination should be made of materials not attenuating radiation doses and should not interfere with the gantry positions that may be required for coplanar and noncoplanar beams.
Respiratory motion management using a number of techniques is frequently needed to minimize imaging artifacts from changes in liver position due to breathing (e.g., active breath hold, abdominal compression). Delineation of target volumes is most often done on multiphasic, multimodality imaging, obtained in breath hold (i.e., similar to diagnostic imaging for HCC). Image-guided radiation therapy (IGRT) is required to account for changes in the liver position day to day. In patients who cannot tolerate active breath control, the use of abdominal compression devices with four-dimensional computed tomography (4DCT) provides information about internal organ motion and can compensate for liver position changes. Gated treatment may also be useful for patients that cannot tolerate breath control.
CT simulation with IV contrast to obtain multiphase imaging is required. This should be obtained with the patient in the treatment position. Fusion of the different phase imaging and/or diagnostic images will aid in the delineation of the gross tumor volume (GTV). Usually the viable HCC is best visualized (brightest) on the arterial-phase CT scan, with less enhancement seen relative to the liver on venous- and delayed-phase imaging. Tumor invasion into the vascular structures (e.g., portal vein or inferior vena cava) is often best observed on either portal-venous- or delayed-venous-phase CT scans.
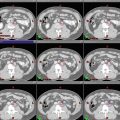
Suggested target volumes for gross disease (GTV) and, in certain circumstances, clinical target volumes (CTV) for high-risk regions are detailed in Table 1 (CTV-macroscopic and CTV-microscopic) (Figs. 1, 2, 3, 4 and 5).
Table 1
Suggest target volumes at the GTV and CTV regions
Target volumes
Definition and description
GTV
Liver tumor: intrahepatic enhancing tumor on arterial-phase contrast CT with washout on venous- or delayed-phase CT
Lipiodol-retaining tumor: lipiodol (white) contiguous to the enhancing tumord
Vascular tumor thrombus: arterial enhancing thrombus with washout on venous-phase CT
CTVmacroscopic a (optional according to clinical indication/protocol)
Liver tumor: the intrahepatic enhancing tumor on arterial-phase contrast CT
Lipiodol-retaining tumor: TACE zone contiguous to the enhancing tumor included in GTV
Enhancing tumor vascular thrombus
CTVmicroscopic (elective) b (optional according to clinical indication/protocol)
3–5 mm margin around intrahepatic GTVc
2–3 mm margin around the tumor thrombus GTV within the vessel
Bland thrombus adjacent to tumor thrombus GTV
Radiofrequency ablation zone adjacent to the GTV
TACE zone not directly adjacent to the GTVRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access