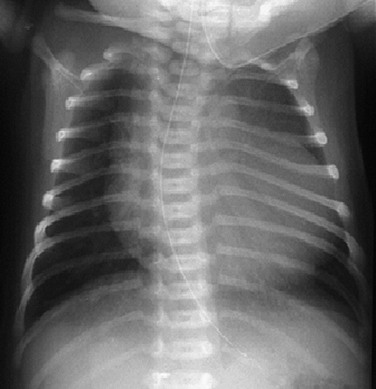
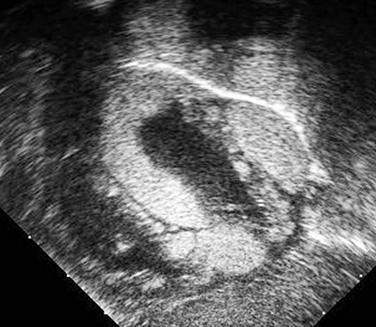
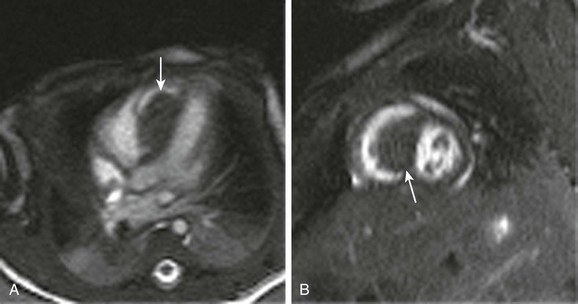
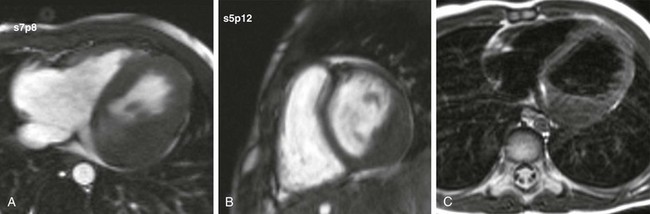
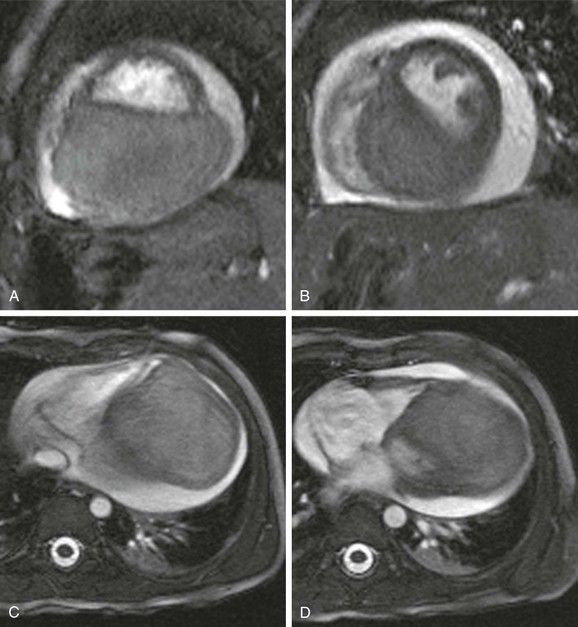
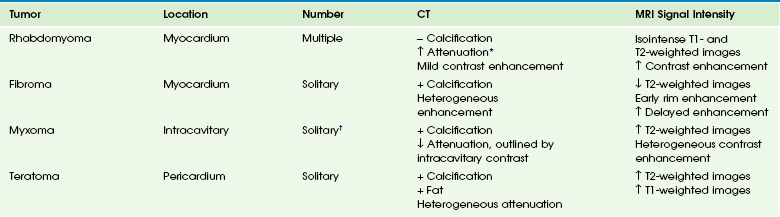
Chapter 81 Primary cardiac tumors are rare in infants and children, with a reported prevalence of up to 0.32%.1 Use of echocardiography has resulted in more frequent detection of cardiac tumors in the fetus and neonate.2 More than 90% of cardiac tumors in infants and children are benign.1 Symptoms are variable and usually depend on tumor location and size. Intracavitary cardiac tumors can cause cardiac valve obstruction or result in spread of tumor emboli into either the pulmonary or systemic vascular beds. Children with intracavitary cardiac tumors present with heart failure, dyspnea, or neurologic symptoms. Myocardial tumors compress the cardiac lumen, leading to obstruction or heart failure, and can be associated with arrhythmias. Pericardial tumors are associated with pericardial effusions. Conventional radiographs may show cardiomegaly, an abnormal cardiac shape, or pulmonary edema from congestive heart failure (e-Fig. 81-1). Cardiac tumors in children can be associated with several syndromes, as shown in Table 81-1. Computed tomography (CT) and magnetic resonance imaging (MRI) findings can help differentiate tumor types (Table 81-2). Table 81-1 Cardiac Tumors Associated with Syndromes Table 81-2 Cardiac Tumors: Computed Tomographic and Magnetic Resonance Imaging Findings CT, computed tomography; MRI, magnetic resonance imaging. †Multiple and recurrent tumors associated with familial forms. Pathophysiology and Clinical Presentation: Rhabdomyoma is the most common primary cardiac tumor of childhood and accounts for 60% to 79% of all cardiac tumors during the first year of life.1,3 Rhabdomyomas are hamartomas that regress and have no potential for malignancy. More than half of fetuses with rhabdomyomas are asymptomatic. Patients with rhabdomyomas can present with nonimmune fetal hydrops, outflow tract obstruction, or arrhythmia. At least 50% of patients with rhabdomyomas have tuberous sclerosis, and rhabdomyomas can be the first detectable manifestation of tuberous sclerosis.3 Imaging: Rhabdomyomas are round, hyperechoic, solid masses on echocardiography (e-Fig. 81-2). They usually are multiple and occur most commonly in the ventricular tissue but also can arise from atrial walls.4,5 The rhabdomyoma signal characteristics on T1- and T2-weighted MRI are similar to those of myocardium, making MRI less sensitive than echocardiography.6 Signal is increased on contrast-enhanced T1-weighted and proton-weighted imaging.7 Rhabdomyomas are easier to detect when they extend into the cardiac lumen (Fig. 81-3). They have increased attenuation compared with myocardium on noncontrast-enhanced CT scans, and they have mild delayed enhancement with contrast (e-Fig. 81-4).8 Small fat globules may be detected in rhabdomyomas. Pathophysiology and Clinical Presentation: Cardiac fibroma is the second most common and the most commonly resected primary cardiac tumor of childhood.9,10 The tumors frequently are detected in the first year of life but can present throughout childhood. Fibromas are solitary tumors located in the myocardium. They are composed of fibroblasts and collagen. Calcifications are frequent and a differentiating finding compared with rhabdomyomas.1,10 The tumor can be associated with Gorlin (basal cell nevus) syndrome.7,9,10 Children can present with heart failure and arrhythmia. Imaging: Echocardiography reveals a heterogeneous, echogenic, solitary mass.10 Cardiac fibroma signal intensity is isointense to slightly hypointense on T1-weighted imaging and low on T2-weighted imaging.9,11 Classically, contrast-enhanced MRI of fibromas initially shows rim enhancement but decreased central enhancement compared with myocardium.12 Enhancement on delayed imaging is characteristic (Video 81-1 and Fig. 81-5 and e-Figs. 81-6 and 81-7).7,13 Calcifications may be detected by CT (e-Fig. 81-8).14 e-Figure 81-6 A solitary left ventricular mass on steady-state free-precession short-axis cine imaging.
Cardiac and Pericardial Tumors
Tumor
Association
Rhabdomyoma
Tuberous sclerosis
Fibroma
Gorlin (basal cell nevus) syndrome
Myxoma
Carney syndrome
Rhabdomyoma
Fibroma
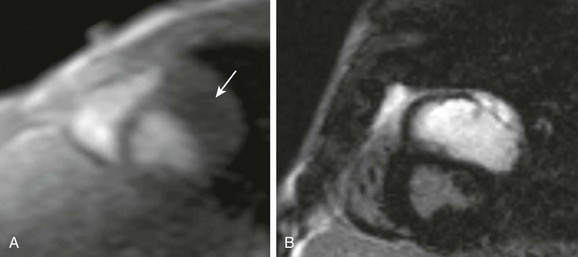
No left ventricular contraction occurs in the region of the fibroma. A, Short-axis first-pass gadolinium perfusion shows no enhancement of the mass (arrow). B, Intense delayed enhancement in the mas is extensive and homogeneous.