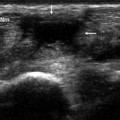
Fig. 9.1
Carpal tunnel syndrome. Macroscopic damage to the median nerve (open arrows in a) is manifested sonographically by enlargement proximal to the point of compression (arrows) (b), hypoechogenicity, and hypervascularity on the color Doppler study (c, d)
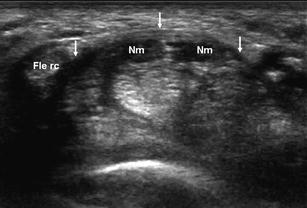
Fig. 9.2
Carpal tunnel syndrome. The bifid median nerve (Nm) is enlarged and hypoechoic; the flexor retinaculum (arrows) is also enlarged with volar bulging; flexor tenosynovitis is also evident
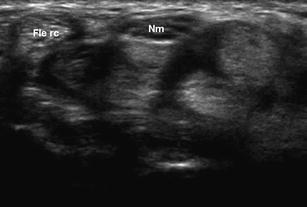
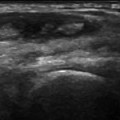
Fig. 9.3
Carpal tunnel syndrome. In this patient with clinically and electromyographically diagnosed carpal tunnel syndrome, sonography reveals flexor tenosynovitis. The absence of macroscopic damage to the median nerve (Nm) is reflected by its normal fasciculated appearance
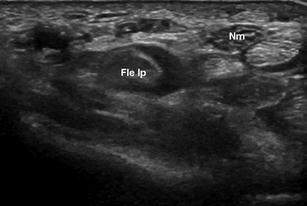
Fig. 9.4
Carpal tunnel syndrome. In this patient with clinically and electromyographically diagnosed carpal tunnel syndrome, sonography reveals tenosynovitis of the flexor pollicis longus (Fle lp) and a median nerve (Nm) with normal fascicular architecture indicating the absence of macroscopic damage
The sonographic examination can often reveal the cause of the symptoms as well, such as flexor tenosynovitis, which is manifested by anechoic fluid at the level of the tendon sheath (Fig. 9.2). When this condition is suspected, dynamic studies are indicated. Images obtained while the patient repeatedly flexes his/her fingers can reveal even small amounts of fluid within the flexor tendon sheath. Dynamic studies also allow assessment of median nerve motility. Sonography can also demonstrate the presence of ganglia (Fig. 9.5) and accessory muscles or tendons (Fig. 9.6) that occupy space and impinge on structures normally present within the tunnel, producing typical symptoms of carpal tunnel syndrome [3–5].

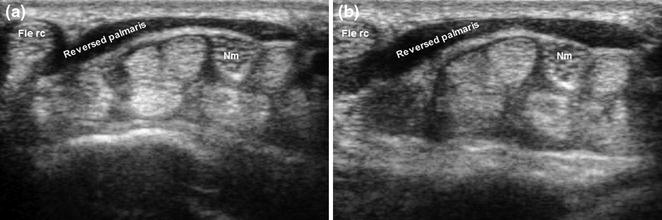
Fig. 9.5
Carpal tunnel syndrome caused by a ganglion cyst. Clinically and electromyographically diagnosed carpal tunnel syndrome. The sonogram reveals a ganglion (arrows) at the level of the carpal tunnel. The median nerve (Nm) retains its normal fascicular appearance (no macroscopic lesions)
Fig. 9.6
Carpal tunnel syndrome associated with a reversed palmaris longus. The sonogram shows a large palmaris longus muscle belly that impinges upon structures in the carpal tunnel whenever the patient flexes his wrist. Flexor tenosynovitis is also evident, but the fascicular architecture of the median nerve (Nm) has been preserved
The syndrome can also be caused by several diseases, including amyloidosis [6, 7




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
