Fig. 1
Diagram illustrating oral cavity subsites
Oral tongue: The oral tongue is the most common site of carcinoma within the oral cavity. It consists of the anterior two-thirds of the tongue and extends posteriorly to the circumvallate papillae, which separate it from the base of the tongue. Squamous cell tumors often arise along the lateral borders of the tongue. Oral tongue tumors may spread to involve the intrinsic and extrinsic musculature, floor of the mouth, neurovascular bundle or mandible.
Floor of the mouth: The floor of the mouth is the second most common subsite. This semilunar space is formed by the mylohyoid, geniohyoid and genioglossus muscles inferiorly. Due to the lack of substantial fascial barriers to spread, floor of the mouth tumors tend to be locally invasive and spread to regional lymph nodes early in their course. The majority of tumors originate near the midline. These can spread laterally into the mandible, superiorly into the ventral tongue and lingual neurovascular bundle, or posteriorly into the base of the tongue. Invasion of the mylohyoid signifies involvement of the submandibular gland, which surrounds the posterior free edge of the muscle. Sublingual spread can obstruct the Wharton duct, leading to duct dilation and submandibular sialadenitis.
Retromolar trigone: The retromolar trigone is a small mucosal region behind the posterior molars. Tumors of this region are associated with a high rate of occult lymph node metastases. Tumors can invade the buccinator, orbicularis oris, or superior constrictor muscles, which insert in this region. They can also spread along the pterygomandibular raphe, reaching the pterygoid plate and base of skull superiorly, or the floor of the mouth inferiorly. They tend to invade bone early. Perineural spread can occur along the inferior alveolar nerve, a branch of CN V3 (Yao et al. 2007) (Fig. 2).
Fig. 2
Anatomy of the inferior alveolar nerve
Alveolar ridge: The alveolar ridges include the maxillary and mandibular alveolar processes and their overlying mucosae. The upper alveolar ridge extends from the upper gingival buccal gutter to the junction of the hard palate and is bordered posteriorly by the upper end of the pterygopalatine arch. The lower alveolar ridge extends from the lower buccal gutter to the line of free mucosa along the floor of the mouth. It is bordered posteriorly by the ascending mandibular ramus. Like tumors of the retromolar trigone, carcinomas of the alveolar ridge tend to invade bone early. Carcinomas of the lower ridge may spread via the mandibular canal and inferior alveolar nerve (Fig. 2). Those of the upper alveolar ridge may invade the maxillary antrum or the base of the nose.
Hard palate: The hard palate is a semilunar space encompassing the inner surface of the superior alveolar ridge to the posterior edge of the maxillary palatine bone. Tumors of the hard palate tend to be confined by the dense mucoperiosteum surrounding it. However, they may invade through exposed areas at the greater palatine foramina or between the primary and secondary palates at the incisive fossa where they can access the nasal cavity. Perineural invasion is most common along the greater palatine nerves, leading to spread along CN V2 from the pterygopalatine fossa through the foramen rotundum to the cavernous sinus and Meckel’s cave (Ginsberg and DeMonte 1998) (Fig. 3).
Fig. 3
Innervation of the hard palate
Buccal mucosa and gingiva: Tumors of the buccal mucosa are rare but tend to be highly aggressive. The buccal mucosa includes the mucosal surfaces of the cheek and lips. This extends to the pterygomandibular raphe posteriorly and to the line of attachment of the mucosa of the upper and lower alveolar ridges superiorly and inferiorly. Tumors may invade the buccinator muscle, the buccal fat pad, or adjacent subcutaneous tissue.
Lip: Most tumors in this region arise at the vermillion border and can spread to adjacent skin or underlying musculature. Lesions located along the gingivobuccal sulcus may erode into the mandibular or maxillary alveolar ridges. Upper lip cancers tend to be more aggressive than those originating in the lower lip.
Lymph node involvement is dependent on several factors, including the subsite and the size of the primary tumor. Retropharyngeal lymph nodes are rarely involved in oral cavity cancer. Lymph node chains routinely involved include levels I–IV (Shah 1990) (Fig. 4).
Fig. 4
Distribution of positive lymph nodes in clinically node negative oral cavity cancer. Shah characterized 65 clinically node negative patients with pathologically positive lymph nodes at the time of radical neck dissection. Numbers indicate the percentage of patients with positive lymph nodes at each anatomic level (Shah 1990)
2 Diagnostic Workup Relevant for Target Volume Delineation
Initial evaluation of suspected oral cavity tumors should involve a thorough history. History taking should focus on risk factors such as tobacco and alcohol use, as well as specific symptoms that may indicate involvement of surrounding structures. Otalgia suggests involvement of branches of CN V3, which innervates the ear via the auriculotemporal branch. Facial numbness can suggest CN V involvement. Trismus can indicate invasion of the pterygoid or masseter muscles.
Physical examination should be performed to help delineate the extent of tumor, which may be beyond what is identified on imaging. Mucosal extent of tumor is often best appreciated on physical examination. This should include inspection and palpation of the oral cavity and neck. Patients should also be referred to a dentist for a complete dental evaluation prior to treatment.
CT can be used as an initial modality to determine the extent of soft tissue destruction and bony involvement, including the pterygopalatine fossa, mandible and hard palate. If CT cannot be obtained, dental panoramas can be used to visualize mandibular involvement.
MRI is critical in the evaluation of perineural spread and is useful in the delineation of the extent of primary tumors. It may also be more helpful than CT if dental artifact makes visualization difficult. T1-weighted images can provide contrast between hypointense tumor and hyperintense bone marrow and fat. However, squamous cell carcinomas are often isointense to muscle on pre-contrast T1-weighted images, making delineation of tumor more difficult in regions such as the oral tongue (Fig. 5). Tumor appears more hyperintense on post-gadolinium T1-weighted images, which can help characterize true bone invasion by tumor (hyperintense) and edema (hypointense) (Hermans 2012). Tumor also appears slightly hyperintense to muscle on T2-weighted images.
Fig. 5
Axial T1-weighted (a), post-gadolinium T1-weighted (b) and T2- weighted (c) MR images, which demonstrate evaluation of a primary oral tongue squamous cell carcinoma. Arrows indicate the location of the primary tumor
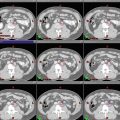
PET imaging is an emerging modality for the evaluation of oral cavity cancers. PET has been shown to be superior to CT and MRI in detecting occult nodal metastasis in oral cavity cancers (Ng et al. 2006). It can also occasionally detect flat tumors that may not be visible on MRI (Fig. 6). PET remains limited, however, in the detection of small metastases and should not be used in isolation.
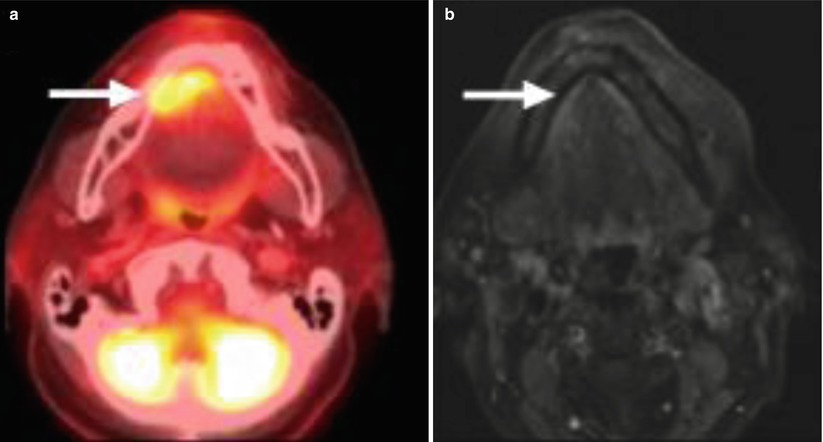
Fig. 6
PET-CT (a) and post-gadolinium T1-weighted MR (b) imaging of a stage T1 floor of mouth squamous cell carcinoma. The tumor is FDG avid on PET but not clearly visible on MRI. Arrows indicate the location of the primary tumor
In the postoperative setting, MRI and PET imaging can be employed to rule out the presence of gross recurrence prior to initiation of treatment. Any suspicious lesions on postoperative imaging should be biopsied, and if positive, surgical re-excision should be considered prior to any course of radiation therapy. Preoperative imaging can help define those regions that should be encompassed in the high-risk CTV.
3 Simulation and Daily Localization
The patient should be simulated in the supine position with the neck in slight hyperextension. A five-point mask should be utilized to immobilize the head, neck, and shoulders. For oral tongue cancers, a bite block can be used during simulation and throughout the course of treatment to elevate the hard palate and decrease dose to the superior oral cavity. For cases in which the hard palate is target, a bite block can be employed to limit dose to the tongue and inferior oral cavity.
CT simulation should be performed using a slice thickness of 3 mm or less. IV contrast is useful in target delineation, particularly with respect to identification of cervical lymph nodes. The patient should be scanned from the top of the head to the carina. The isocenter is typically placed just superior to the arytenoids.
If available, MRI or PET scans obtained at the time of simulation can often be helpful in defining target volumes.
The tumor volumes and normal tissue volumes should be outlined on all CT slices on which the structures exist. Image guidance should be used to verify patient positioning during treatment. We favor daily kV imaging, which can minimize setup error and allow for smaller PTV margins. Setup uncertainty is typically greatest in the mental region, which is farthest from the pivot point for neck rotation.
4 Target Volume Delineation and Treatment Planning
The GTV70 is defined as all known gross disease, as determined by CT, MRI, PET and physical examination. This volume includes all grossly positive lymph nodes, which are those measuring >1 cm, containing a necrotic center or FDG avid on PET imaging. The high-risk CTV70 is typically identical to the GTV70, although a margin of 5 mm can be added if uncertainty exists regarding the extent of gross disease.
For definitive cases, an intermediate-risk volume (CTV59.4)) encompasses an additional margin around the primary tumor, including potential sites of spread. Nodal levels at high risk for microscopic disease are also included in the CTV59.4. Those nodal levels at lower risk are encompassed by the CTV54.. See Tables 1 and 3 for details.
Table 1
Suggested target volumes for definitive treatment of oral cavity cancers
Target volumesa
Definition and description
GTV70
Primary: all gross disease on physical examination and imaging
Neck nodes: all gross disease and physical examination and imagingRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access