Mucosal hyperenhancement accompanies active ulceration
Reversal of jejunoileal fold patterns (atrophied jejunal, thickened ileal)
Submucosal edema, fat, or gas
Small bowel intussusception
Eccentric soft tissue density mass in bowel wall (tumor)
Mesenteric adenopathy (may be cavitated)
• Excess fluid within SB lumen
Conformation of flaccid SB segments
Distends lumen and dilutes contrast medium
• Colonic luminal dilation
Excess gas, fluid, fat within lumen
• Eccentric soft tissue density mass in bowel wall
Strongly suggests lymphoma or carcinoma
TOP DIFFERENTIAL DIAGNOSES
• Whipple disease
• Crohn disease
• Intestinal opportunistic infections
CLINICAL ISSUES
• Common: Affects 1 in 200 in USA, but < 10% are currently diagnosed
Most common cause of SB disease and malabsorption
• Steatorrhea, abdominal distension, flatulence
Diarrhea, weight loss, glossitis, anemia
• Refractory disease
Enteritis that does not respond to at least 6 months of gluten-free diet
GI malignancies are main cause of death in celiac disease
(Left) Axial CECT in a 37-year-old man with painful abdominal cramps shows 1 of several sites of intussusception , typically short segment and nonobstructing.
(Right) Axial CECT in the same patient demonstrates that the jejunal fold pattern seems blunted. Also noted is mesenteric lymphadenopathy .
(Left) Axial CECT in the same patient shows more mesenteric lymphadenopathy along with the abnormally blunted jejunal fold pattern.
(Right) Axial CECT in the same patient shows another intussusception . There is a suggestion of abnormal fold prominence in the ileum . The flaccid, dilated pelvic SB loops press on each other without intervening space, known as the conformation sign.
TERMINOLOGY
Synonyms
• Nontropical sprue or celiac-sprue disease, gluten-sensitive enteropathy
Definitions
• Celiac disease: Chronic intolerance of gluten that induces intestinal injury in genetically predisposed individuals
• Tropical sprue: Malabsorption seen in inhabitants of tropical countries
IMAGING
General Features
• Best diagnostic clue
CT enterography: Evidence of reversed fold pattern, multifocal intussusception
• Location
Celiac disease: More proximal small bowel
Tropical sprue: Entire small bowel
• Other general features
Most common small bowel disease producing malabsorption syndrome
Due to sensitivity of small bowel to α-gliadin
– Component of gluten
Has familial susceptibility with genetic basis
Radiographic Findings
• Barium small bowel follow-through (SBFT)
Dilatation of small bowel (jejunum): > 3 cm
Valvulae conniventes: May exhibit 5 patterns
– Valvulae look normal in most patients
– Ends at margin that are squared off rather than rounded
– Reversed jejunoileal fold pattern: ↓ number of jejunal folds and ↑ ileal folds
– Blunted or absent valvulae: “Moulage” sign (cast): Characteristic of sprue
– Thickening: In severe disease and hypoproteinemia
“Colonization of jejunum”: Loss of jejunal folds → colon-like haustrations
Hypersecretion-related artifacts: Due to excess fluid
– Flocculation: Coarse granular appearance of small clumps of disintegrated barium due to excess fluid; mainly in patients with steatorrhea
– Segmentation: Break up of normal continuous column of barium, creating large clumps of barium separated by string-like strands
Transit time: May be long, short, or normal
Nonpropulsive peristalsis (flaccid and poorly contracting bowel loops)
Painless, transient intussusceptions often seen on fluoroscopic studies
• Fluoroscopic-guided enteroclysis
More accurate than SBFT in diagnosing celiac disease
Jejunal folds
– Decreased number of proximal jejunal folds (< 3/inch; normal: ≥ 5/inch)
– Increased separation and absence of folds; “ileal” appearance
Ileal folds
– Increased number of folds in distal ileum (4-6/inch; normal: 2-4/inch)
– Increased fold thickness ≥ 1 mm: “Jejunization” of ileum in 78% of cases
Mosaic pattern: Due to total villous atrophy
– 1-2 mm islands of mucosa surrounded by barium-filled grooves
Duodenal changes
– Decreased number and irregular folds, especially in distal duodenum
– “Bubbly” duodenum: Nodular pattern in mucosa
CT Findings
• Excess fluid within SB lumen
Distends lumen and dilutes positive enteric contrast medium
• SB wall may be thick or thinned
Mucosal hyperenhancement accompanies active ulceration
Submucosal edema; halo sign
Submucosal fat in wall of duodenum and jejunum
Pneumatosis has been reported (not due to ischemia)
Only gold members can continue reading. Log In or Register to continue













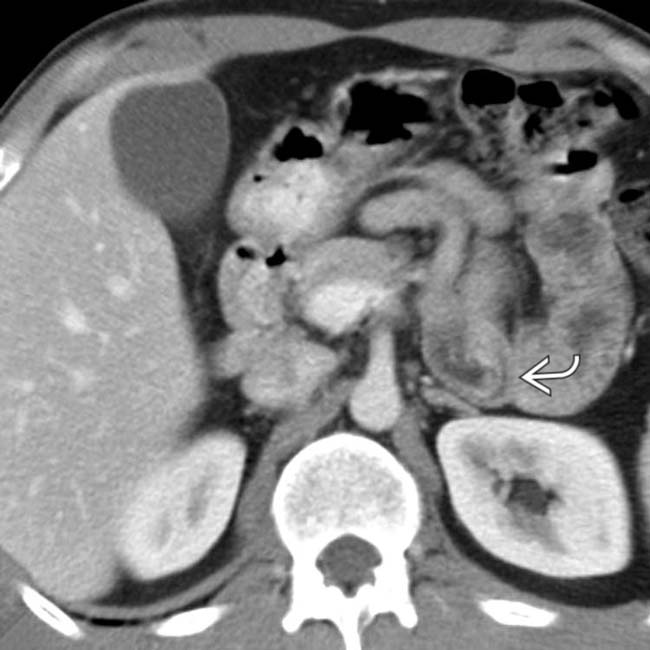
 , typically short segment and nonobstructing.
, typically short segment and nonobstructing.
 .
.
 along with the abnormally blunted jejunal fold pattern.
along with the abnormally blunted jejunal fold pattern.
 . There is a suggestion of abnormal fold prominence in the ileum
. There is a suggestion of abnormal fold prominence in the ileum  . The flaccid, dilated pelvic SB loops press on each other without intervening space, known as the conformation sign.
. The flaccid, dilated pelvic SB loops press on each other without intervening space, known as the conformation sign.





 Hypersecretion-related artifacts: Due to excess fluid
Hypersecretion-related artifacts: Due to excess fluid





















