Radiologic evaluation of neoplasms in the central skull base can be challenging as primary and secondary osseocartilaginous neoplasms as well as invading masses from adjacent intracranial and extracranial compartments can all affect this anatomically complex region. Nonneoplastic pathologies may mimic malignancies in the central skull base, which is difficult to reach by percutaneous biopsy and contains numerous sensitive neurovascular structures. This article will review the anatomy of the central skull base, provide an anatomically oriented approach to organizing differentials for central skull base masses, and illustrate classic imaging features of common neoplasms encountered in this region.
Key points
-
•
Neoplasms that arise in and around the central skull base can cause multiple cranial neuropathies and vascular complications due to the high number of important neurovascular structures in the region.
-
•
With a thorough understanding of normal central skull base anatomy, high quality radiological differential diagnoses can be generated in this difficult-to-biopsy area.
-
•
Careful analysis of tumor location and mass effect on surrounding structures, as well as computed tomography and MR imaging features of central skull base masses can help refine the imaging differential.
Abbreviation
| PitNET | pituitary neuroendocrine tumor |
Introduction
The central skull base is an anatomically complex osseous structure, which borders multiple important extracranial and intracranial spaces and contains numerous critical vessels and nerves. Dedicated MR imaging and CT imaging protocols are often complementary when evaluating tumors in this region, which can be challenging as primary and secondary osseous neoplasms as well as invading masses from adjacent intracranial and extracranial compartment tissues can all affect the central skull base. Furthermore, vascular, infectious, inflammatory, and developmental pathologies may also mimic neoplasms in this area, which is difficult to reach by percutaneous biopsy.
This article will first briefly discuss modality and protocol considerations of central skull base imaging, then review the relevant anatomy before providing an anatomically oriented approach to organizing differential diagnoses for central skull base neoplasms. Pathologies will be discussed based on their site of origin, with the first section focusing on intracranial neoplasms invading down into the central skull base, the second focusing on primary or secondary osseous neoplasms that originate from the sphenoid and clivus, and the third focusing on extracranial neoplasms extending upward into the central skull base. Characteristic radiological findings of each entity will be described and illustrated with classic case examples.
Imaging modalities and considerations
MR imaging and CT modalities offer complementary evaluation of central skull base tumors, as CT is necessary for detailed evaluation of osseous involvement and MR imaging is superior in the evaluation of tissue characteristics and extent. CT protocols should include submillimeter images in bone and soft tissue reconstruction algorithms to allow for multiplanar reconstruction. Dedicated skull base MR imaging protocols should include T1-weighted (nonfat-suppressed), T2-weighted fat-suppressed, and postcontrast T1-weighted fat-suppressed images in axial and coronal planes, with slice thicknesses no more than 3 mm, covering the skull base and surrounding structures. In the skull base, an area that is prone to local magnetic field inhomogeneities, Dixon fat suppression technique offers more uniform imaging quality than conventional chemical shift fat suppression. Diffusion imaging can help identify and characterize cellular tumors and potentially aid in the distinction between chondrosarcomas and chordomas. , 3-dimensional postcontrast sequences or heavily T2-weighted sequences (CISS, FIESTA, or T2-SPACE) should be considered when there is clinical concern for cranial nerve palsies, where increased spatial resolution may help detect perineural tumor or characterize nerve compression. The additional information any given MR imaging sequence might yield must be balanced against the fact that a longer examination is more likely to be rendered nondiagnostic by motion artifact. Thus, communication with referring providers and understanding of patient tolerance may help tailor a most diagnostic protocol while minimizing scan time.
Anatomy
The osseous skull base is divided into anterior, central, and posterior portions. While there are no uniformly agreed upon, strict anatomic boundaries to the central skull base, it is commonly defined as being composed of the body and medial portions of the greater wings of the sphenoid bone and petrous apices of the temporal bones. The sphenoid body contains the sphenoid sinuses and abuts the bilateral cavernous sinuses, forming the upper portion of the clivus. Superiorly, it contains the sella turcica, which houses the pituitary gland. The sella is bounded by the tuberculum sellae anteriorly and dorsum sellae posteriorly and surrounded by 4 bony projections of the sphenoid body, the paired anterior and posterior clinoid processes ( Fig. 1 A–C). The greater wings of the sphenoid, extending from the inferior aspect of the body, form the anterior inferior boundaries of the middle cranial fossa bilaterally and portions of the central skull base, through which important foramina including the foramen rotundum, foramen ovale, and foramen spinosum traverse. Further posteriorly, the anterior aspects of the petrous ridges of the temporal bones form the boundary between the middle and posterior cranial fossa. The petrous apices are the pyramid-shaped, anteromedial projections of the temporal bones that meet the clivus at the petro-clival/petro-occipital junctions.
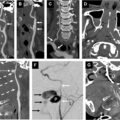
Major osseous structures and neuroforamina of the central skull base. ( A, B ) 3D CT reconstructions of the intracranial surface of the osseous central skull base, viewed craniocaudally, illustrate anterior clinoid process ( circle ), posterior clinoid process ( square ), foramen ovale ( blue arrow ), foramen spinosum ( blue arrowhead ), foramen lacerum ( white arrowhead ), petrous apex ( black square ), optic canal ( orange arrowhead ), sella (S), clivus (C), cavernous sinus ( arrow ), including cavernous ICA, basilar artery ( dashed arrow ), supraclinoid ICA ( black arrowhead ), middle cerebral artery ( red arrowhead ), anterior cerebral artery ( yellow arrowhead ), and posterior cerebral artery ( green arrowhead ). ( C ) 3D CT reconstruction of the extracranial surface of the osseous central skull base, viewed anteroposteriorly, illustrates superior orbital fissure ( circle ), inferior orbital fissure ( arrowhead ), foramen rotundum ( dashed arrow ), vidian canal ( black arrows ), sphenoid sinus (S), pterygoid (P), greater (G) and lesser (L) sphenoid wings, and vomer ( white arrow ).
Multiple neuroforamina and vascular foramina in the central skull base contain critical neurovascular structures and serve as conduits between the extracranial space and the intracranial space ( Table 1 ). Tumors can directly arise from the contents of these conduits or spread through them and can cause a broad range of cranial nerve palsies and vascular complications.
Table 1
Major neurovascular structures traversing the central skull base
| Skull Base Structure | Major Neurovascular Contents |
|---|---|
| Optic nerve canal | Optic nerve (CN II) and ophthalmic artery |
| Dorello canal | Abducens nerve (CN VI) |
| Vidian canal | Vidian nerve and artery |
| Carotid canal | Sympathetic plexus and petrous ICA |
| Superior orbital fissure | Oculomotor nerve (CN III), trochlear nerve (CN IV), ophthalmic branch of the trigeminal nerve (CN V1), abducens nerve (CN VI), and superior ophthalmic vein |
| Foramen rotundum | Maxillary division of the trigeminal nerve (CN V2) and artery of the foramen rotundum |
| Foramen lacerum | Greater and deep petrosal nerves, lacerum ICA, and ascending pharyngeal artery branches |
| Foramen spinosum | Meningeal branch of the mandibular nerve and middle meningeal artery and vein |
| Foramen ovale | Mandibular division of CN V3, otic ganglion, lesser petrosal nerve, and accessory meningeal artery |
Abbreviation: CN, cranial nerve; ICA, internal carotid artery.
A thorough understanding of central skull base anatomy is imperative to the development of appropriate differential diagnoses when faced with tumors in this area. Broadly, the central skull base neoplasm can be separated into 3 main categories: those that arise intracranially and invade downwards into the osseous skull base, those that arise directly from the osseous skull base and/or the neurovascular structures passing through it, and those that arise extracranially and invade upwards into the osseous skull base. The first step toward categorizing a mass that crosses multiple compartments is identifying the center of the mass and placing it either intracranially, in the bony skull base, or extracranially. This categorization can be further supported by the analysis of the pattern of osseous erosion or remodeling, as well as the displacement of key anatomic and neuroforaminal landmarks ( Fig. 2 A–C). Finally, recognition of the normal entities that exist in each anatomic location will help narrow the differential considerations once the center of a neoplasm is identified.
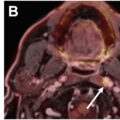
Sagittal CT head of ( A ) a 50-year-old female with pituitary adenoma, ( B ) a 70-year-old male with osseous metastasis from colon cancer, and ( C ) a 56-year-old female with nasopharyngeal cancer demonstrate characteristic osseous erosion patterns of intracranial versus intraosseous versus extracranial origin neoplasms. ( A ) Intracranial origin tumors ( white circle ) tend to center above the osseous skull base or are inseparable from native intracranial structures, causing erosion of the inner cortex of the clivus and enlargement of the sella ( black arrowhead ). ( B ) Intraosseous origin tumors ( black square ) tend to center in the bone, expanding and eroding both dorsal and ventral cortices of the clivus ( white arrowheads ). ( C ) Extracranial origin tumors ( white square ) are centered extracranially and preferentially erode the ventral clival cortex ( white arrow ).
Pathologies
Intracranial Tumors Affecting the Central Skull Base
In general, intracranial neoplasms that invade into the central skull base are centered above the level of the skull base and tend to expand the spaces they occupied intracranially before eroding into bone. When invading into the skull base, many intracranial neoplasms take the path of least resistance , preferentially extending through and widening preexisting fissures and neuroforamina. This may result in characteristic dumb-bell shaped tumors above and below the constrictive bony skull base.
Sellar masses
Pituitary neuroendocrine tumor (PitNET), previously known as pituitary adenoma, can be locally invasive. The invasive PitNET should be the foremost differential consideration when a central skull base mass appears inseparable from the pituitary gland and what remains of the sella is widened. PitNETs can invade through the floor of the sella into the osseous clivus, sphenoid sinuses, and cavernous sinuses without significant suprasellar extension, but there is usually some component of the mass that occupies the expected location of the sella, between the anterior and posterior clinoid processes. PitNET typically displays delayed hypo-enhancement relative to normal pituitary tissue, and can demonstrate internal heterogeneity, fluid-fluid levels, and intrinsic T1 hyperintensity related to hemorrhage ( Fig. 3 A–C).
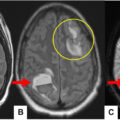
50-year-old female with vision loss. Sagittal midline precontrast ( A ) and postcontrast ( B ) T1 weighted imaging (T1WI) demonstrate a heterogeneous mass, with precontrast T1 hyperintense hemorrhagic component superiorly ( circle ) and enhancing tumoral component inferiorly ( square ). Tumor is centered intracranially within the suprasellar cistern, expands sella ( white triangle ) with invasion into the sphenoid sinus (S). Coronal T2 weighted imaging (T2WI) ( C ) shows tumor superiorly displaces optic chiasm ( white arrow ), and invades the right cavernous sinus ( arrowhead ) without narrowing of the vascular lumen of the ICA ( white asterisk ) or the posterior communicating artery ( white arrowhead ). The mass is inseparable from the pituitary gland and compatible with an invasive PitNET/macroadenoma.
Germ cell tumors or isolated metastatic lesions arising from the sellar contents can also cause erosion of the skull base, although these entities are much rarer than PitNETs. Craniopharyngiomas, which are most often suprasellar in origin, can extend inferiorly and rarely cause remodeling and erosion of the skull base.
Meningioma
Meningiomas are commonly found in the skull base, with approximately half of all meningiomas presenting in this location. , The dural reflections along the petroclival, paraclinoid, and pericavernous regions of the central skull base are common locations for meningiomas, and even small tumors in these critical areas of high neurovascular concentration can be symptomatic. Petroclival meningiomas often grow infiltratively along the dural surfaces of the tentorial leaflets and may cause mass effect on the posterior and middle cranial fossa contents, including the brainstem and cranial nerves in the prepontine cisterns and Meckel’s caves. Anteriorly, petroclival meningiomas and paraclinoid meningiomas can grow into the sella, cavernous sinus, optic canal, and orbital apex, causing multiple cranial neuropathies and optic nerve compression. When meningiomas involve the cavernous sinus and encase the carotid artery, they can cause narrowing of the vessel lumen, distinguishing them from PitNETs. Due to the anatomic complexity of this region and the critical structures that may be impacted, accurate radiological tumor mapping is imperative in definitive surgical and radiation treatment planning.
Skull base meningiomas are usually sessile lesions with a broad-based dural attachments, uniform avid enhancement and characteristic dural tails ( Fig. 4 A, B). Meningiomas can demonstrate hyperperfusion on MR perfusion techniques such as arteral spin labeling (ASL). Nearly 90% of meningiomas will cause hyperostosis of the underlying bones, best demonstrated on CT, which may contribute to mass effect on adjacent neuroforaminal contents. They can extend extracranially through skull base neuroforamina, including the foramen rotundum and ovale. Occasionally, this may result in a dumb-bell shaped mass, which might mimic a schwannoma. In rare cases, meningiomas may cause lytic osseous erosion and mimic metastatic disease and multiple myeloma. It is important to note that radiologic features of adjacent brain parenchymal edema, osseous and dural invasion cannot reliably distinguish benign (World Health Organization [WHO] grade I), atypical (WHO grade II), and malignant/anaplastic (WHO grade III) meningiomas. ,
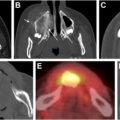
47-year-old woman with gradual proptosis. ( A ) Axial CT demonstrates extensive hyperostosis and expansion of the left sphenoid body and greater wing ( arrows ) and left globe proptosis (P). ( B ) Axial postcontrast T1WI demonstrates avidly enhancing en plaque meningioma associated with the hyperostosis, extending into the left orbit ( circle ), infratemporal fossa ( square ), sphenoid sinus ( dashed white arrow ), and foramen rotundum ( arrowhead ). Surgical debulking demonstrated atypical meningioma (WHO grade II).
Schwannoma
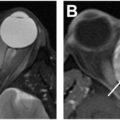
Schwannomas are common benign peripheral nerve sheath tumors which, in the central skull base, most commonly involve the maxillary and mandibular divisions of the trigeminal nerve ( Fig. 5 A–C). They grow along the expected normal anatomic paths of their associated nerves, from the intracranial cisternal segment through skull base neuroforamina to the extracranial space. They characteristically appear as tubular or dumbbell-shaped masses with distinct, smooth margins. Due to their benign, slow growing nature, schwannomas are associated with smooth remodeling and expansion of the neuroforamina with thinned yet preserved cortex. On MR, they are typically T1 hypointense, T2 hyperintense, with heterogeneous enhancement and possible internal cystic or hemorrhagic components.
26-year-old woman with an incidental skull base mass after neuroimaging performed for trauma. ( A ) Coronal postcontrast T1WI demonstrates a large expansile mass ( asterisk ) of the left central skull base, extending into the left middle cranial fossa and masticator space along the expected location of the V3 trigeminal nerve, with characteristic dumbbell-shaped constriction at the expanded foramen ovale ( white arrowheads ), ( B ) Axial T2WI, and ( C ) axial CT show the mass ( asterisk ) demonstrating heterogenous T2 signal intensity, effacing the pterygopalatine fossa ( white arrows ), petrous apex and carotid canal ( dashed white arrows ). Despite its large size, the mass is well-circumscribed with a benign osseous remodeling/thinning and expanding the bony cortex of the pterygoid base ( black arrowheads ). Surgical debulking revealed a schwannoma.
Tumors Arising from the Osseous and Fibrocartilaginous Central Skull Base
In general, tumors arising from the osseous and fibrocartilaginous central skull base are inseparable from the bony clivus. They may expand outwards into the intracranial and/or extracranial compartments, but the center of the mass remains within what would be the normal confines of the bony structures. When extending intracranially, these tumors tend to narrow or displace normal intracranial spaces, such as the sella or the Meckel’s caves. Similarly, they typically cause narrowing, rather than expansion, of the skull base neuroforamina.
Chordoma
Chordomas are slow-growing malignant primary tumors arising from embryonic remnants of the notochord that are commonly found along the spinal axis, especially in the sacrum. Chordomas arising from the skull base comprise 39% of all chordomas, and majority occurs in midline clivus. , While most chordomas are low-grade and classified as conventional, other less frequently occurring subtypes include chondroid, poorly differentiated, and dedifferentiated, and may have a more aggressive pattern of growth. Clinically, skull base chordomas usually present with the symptoms related to neurovascular compression. ,
On CT, chordomas typically present as well-defined, expansile lytic clival mass, , with preferential dorsal extension into the prepontine cistern and exhibit the thumb sign (indentation of the ventral pons). Internally, the mass may demonstrate areas of scattered bony sequestrum/calcification. On MR, chordomas typically appear T2 hyperintense, though there may be areas of scattered internal heterogeneity on precontrast T1WI and T2WI due to the presence of mucin and intratumoral hemorrhage ( Fig. 6 A–C). It typically demonstrates low-level enhancement and comparatively lower apparent diffusion constant (ADC) values on diffusion-weighted imaging (DWI) than chondrosarcoma. ,