Accurate staging of oral cavity cancer is essential for guiding appropriate treatment and predicting patient outcomes. Radiology plays a pivotal role in this process by providing critical information on tumor size, nodal involvement, and potential spread to adjacent structures—key parameters in the staging and management of the disease.
Key points
-
•
Imaging plays a critical role in preoperative staging of oral cavity cancers.
-
•
Clinical examination is a cornerstone of initial assessment of oral cavity cancer, but imaging plays a crucial role in evaluating extent of tumor, nodal involvement, bone invasion, and potential perineural spread of tumor.
-
•
With advances in multimodality imaging, radiologists are increasingly able to provide detailed anatomic information that complements histopathology.
Abbreviations
| ADC | apparent diffusion coefficient |
| AJCC | American Joint Committee on Cancer |
| CT | computed tomography |
| DOI | depth of invasion |
| ENE | extra-nodal extension |
| FDG | fluorodeoxyglucose |
| RMT | retromolar trigone |
| TT | tumor thickness |
Oral cavity cancer— Why do we stage
There are an estimated 58,000 new cases and 12,000 deaths attributed to oral cavity or oropharyngeal cancer annually in the United States. Oral cavity cancer—most of which is squamous cell carcinoma—is the sixth most common cancer worldwide accounting for approximately 300,000 new cases each year. ,, These cancers are twice as common in men as in women, with the highest prevalence observed in middle-aged men, averaging around 64 years of age. ,, However, recent years have shown a rising incidence among younger populations, with approximately 20% of cases now occurring in individuals under the age of 55 years. , Additionally, the overall incidence among women is increasing, largely driven by a rise in oral tongue primaries. Approximately 40% of cases of oral cavity cancers arise from the oral tongue, followed by primary tumors of the lip (∼16%), floor of mouth (∼16%), gum (∼10%), buccal mucosa (∼7%), retromolar trigone (RMT; ∼6%), and hard palate (∼2%). About 40% to 60% of oral cavity cancers present at advanced stages (stages III or IV) at the time of diagnosis. Metastases to cervical lymph nodes are seen in up to 45% of cases upon initial presentation.
The significance of accurate staging of oral cavity cancer cannot be overstated—it directly influences treatment decisions and outcomes. The staging of oral cavity cancer provides a framework for prognostication and applying guidelines for treatment and management. The concepts of describing cancer as local, regional, and distant began to take shape in the early 1900s and have developed into the modern TNM staging system. The role of imaging is critical in staging of oral cavity cancer and determining the best treatment approaches to optimize patient outcomes. Evidence-based guidelines are often tied to specific stages of cancer and imaging plays a pivotal role in this determination. Staging helps estimate a patient’s prognosis allowing for better informed discussions about outcomes and planning. Patients can be matched to clinical trials based on cancer stage, improving access to innovative therapies. Lastly, staging aids in evaluating the success of treatment and planning follow-up care including monitoring for recurrence.
Oral cavity anatomy— where
The oral cavity is a space defined inferiorly by the mylohyoid muscle, anteriorly by the alveolar ridge and teeth, laterally by the gingivobuccal regions, posteriorly by the circumvallate papillae of the tongue, and superiorly by the hard palate, maxillary alveolar ridge, and teeth. The mylohyoid forms the floor of the oral cavity, and the hard palate forms the roof. The buccal mucosa lines the inner cheeks and reflects superiorly over the maxilla and inferiorly over the mandible.
The oral cavity proper is further subdivided into the oral tongue (anterior two-thirds of the tongue), the floor of mouth, and the sublingual and submandibular spaces. The posterior one-third of the tongue is the base of tongue, delineated by the circumvallate papillae, and it is a subsite of the oropharynx rather than the oral cavity ( Fig. 1 ).
The oral cavity including the oral tongue ( purple ) is anterior to the oropharynx which includes the base of tongue ( green ).
( Courtesy of Kelly Kage, MFA, CMI, Houston, TX.)
The oral tongue consists of the intrinsic and extrinsic muscles. The intrinsic muscles lack bony attachments and include the inferior and superior longitudinal muscles and the transverse, vertical, and transverse lingual muscles. In contrast, the extrinsic muscles of the tongue do have bony attachments and originate outside of the tongue itself. The extrinsic muscles include the genioglossus, styloglossus, and hyoglossus, innervated by the hypoglossal nerve, and the palatoglossus, innervated by the pharyngeal branch of the vagus nerve. The genioglossus muscle arises from the superior mental spine of the inner surface of the mandible and fans out along the inferior aspect of the tongue. The paired genioglossus muscles are divided by the midline lingual septum and function to protrude the tongue. The styloglossus muscle elevates the lateral aspects of the tongue to create a channel for swallowing. It arises from the styloid process of the petrous temporal bone and is attached to the stylomandibular ligament. The hyoglossus muscle runs along the length of the hyoid bone and inserts into the side of the tongue where it serves to retract the tongue ( Fig. 2 ). Due to its close anatomic proximity to key neurovascular structures, including the hypoglossal nerve (CN XII), lingual artery and nerve, the hyoglossus muscle is an important surgical landmark. The fourth extrinsic muscle of the tongue, the palatoglossus, elevates the posterior tongue to initiate swallowing. The palatoglossus arises from the lateral aspect of the soft palate and interdigitates with the intrinsic tongue muscles at the lateral tongue margin.
Axial T1 image shows the genioglossus muscle ( yellow arrow ), hyoglossus muscle ( red arrow ), and sublingual gland ( light blue arrow ).
The floor of mouth is bordered by the mylohyoid muscle inferiorly, tonsillar pillars posteriorly, and the mandible anteriorly. The mylohyoid muscle, innervated by a branch of V3, originates from the mylohyoid ridge of the mandible and extends posteriorly to the last molar. , The anterior bellies of the digastric muscle which run inferiorly under the mylohyoid provide additional support to the floor of mouth. ,
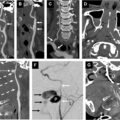
The RMT ( Fig. 3 ) is a triangular mucosal covered region of the oral cavity that is bounded anteriorly by the last mandibular molar, posteromedially by the anterior tonsillar pillar, and laterally by the buccal mucosa. Despite its small size, the RMT is a clinically significant anatomic location due to its strategic location and potential pathways for tumor spread. Tumors in this location can readily spread to the oropharynx and can spread along the pterygomandibular raphe. This route facilitates infiltration into the deeper soft tissues, complicating both surgical resection and prognosis.
The retromolar trigone of the oral cavity is a small space but may provide a pathway for deeper spread of oral cavity cancers. The pterygomandibular raphe may facilitate spread of tumors into the oropharynx or masticator space.
( Courtesy of Kelly Kage, MFA, CMI, Houston, TX.)
The pterygomandibular raphe (see Fig. 3 ) is a fibrous band that lies deep to the RMT and extends from the hamulus of the medial pterygoid to the mandibular mylohyoid ridge with attachments to the buccinator and superior pharyngeal constrictor muscles. Although not well seen on imaging, awareness of the pterygomandibular raphe is crucial in evaluating oral cavity cancers. Tumor involvement of this fibrous band may facilitate extension to the oropharynx or the masticator space, potentially necessitating a more aggressive surgical approach and impacting overall staging and prognosis.
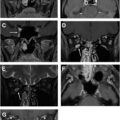
The sublingual space is bounded inferiorly and laterally by the mylohyoid, anteriorly by the mandible, and medially by the geniohyoid and genioglossus muscles ( Fig. 4 ). The lingual nerve of V3, lingual artery and vein, hypoglossal nerve and the sublingual glands and ducts run in the sublingual space. The deep portion of the submandibular gland and Wharton’s duct also extend through the sublingual space. , The sublingual space is separated from the submandibular space by the mylohyoid anteriorly, but the two spaces are contiguous posteriorly.
Anatomic structures of the oral cavity are shown in this coronal diagram.
( Courtesy of Kelly Kage, MFA, CMI, Houston, TX.)
Staging the primary—how
In the most recent 8th edition of the American Joint Committee on Cancer (AJCC) staging manual for oral cavity cancer, one of the most significant changes for T staging from the prior edition was the removal of extrinsic tongue muscle involvement as a staging criterion. This was replaced by the inclusion of depth of invasion (DOI) as a more reliable prognostic factor. DOI is defined as the distance from basement membrane to the deepest point of tumor on histopathological evaluation. This is in contrast to tumor thickness (TT) which has been variably defined. TT has shown an association with nodal disease, with TT greater than 4 mm having a positive association with cervical nodal disease. More recently, reports have suggested there is not a significant difference in prognostication when using either DOI or TT in T staging.
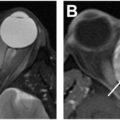
Computed tomography (CT) does not reliably predict DOI ( Figs. 5 A, B and 6 A, B ). MR imaging has demonstrated the ability to predict DOI in tongue squamous cell carcinoma (SCC), with some studies showing good correlation between MR imaging and histopathologic DOI, although MR imaging may tend to overestimate DOI. MR image-based DOI has been assessed on one study by measuring the distance from the normal mucosa adjacent to the tumor to the deepest point of invasion on axial T1-weighted and T2-weighted images. T2-weighted imaging may overestimate DOI to a greater extent than T1-weighted imaging, as peritumoral edema may be included in the measurement on T2-weighted images.
Tumor thickness on ( A ) coronal post-contrast CT neck of this right lateral tongue SCC ( red arrow ) measured 8 mm. ( B ) Axial post-contrast CT shows the right lateral tongue SCC ( red arrow ). This was an overestimate of the pathologic DOI which measured 2 mm.
( A ) Axial post-contrast CT shows a right lateral tongue SCC ( red arrow ). ( B ) Coronal CT image shows TT measuring 1.4 cm which was close to the pathologic DOI of 1.6 cm.
Intraoral ultrasonography, particularly ultra-high frequency ultrasound, has been used both preoperatively and intraoperatively to evaluate DOI and TT. Pre-operative intraoral ultrasonography measurements of DOI and TT correlate strongly with gold standard histopathologic measurements of DOI and TT. ,,, Studies in patients with oral cavity SCC showed that CT and MR imaging may both overestimate histologic DOI, with ultrasound (US) DOI measurements more often accurate, especially in thin tumors. ,, Correlation between US DOI and histopathologic DOI is particularly strong in T1-T2 stage oral tongue cancers. ,,
Bone invasion is an upstaging feature when staging oral cavity SCC. When evaluating bone invasion, MR imaging demonstrates high sensitivity but lower specificity compared to CT. Contrast-enhanced CT has the highest specificity for the assessment of cortical bone involvement and erosion. , Bone invasion is associated with a worse prognosis and is a key factor in surgical planning. Fluorodeoxyglucose (FDG) uptake on PET CT has not been shown to improve identification of bone invasion compared to contrast-enhanced CT alone. However, single-photon emission CT has shown pre-operative value in effectively ruling out mandibular invasion of oral SCC, aiding in resection planning. Assessment of bone involvement on pre-operative imaging is critical, as it can be difficult to determine clinically and through frozen section pathology. Resection margins are a crucial prognostic factor that directly impacts survival and recurrence rates.
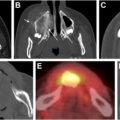
Certain subsites, such as gingivobuccal and RMT tumors, have a higher incidence of bone involvement; therefore contrast-enhanced multidetector CT is the preferred imaging modality for initial assessment. ,, Techniques such as puffed cheek technique during CT acquisition aid in detection of the primary tumor ( Figs. 7–9 ). A main limitation of CT evaluation of the oral cavity is artifact from dental amalgam. Image quality can be improved using a second pass CT with angled gantry and the application of metal reconstruction algorithms.
Post-contrast CT shows normal mucosal surfaces of the buccal space and gingiva are well shown on puffed cheek technique. ( A ) Coronal image. ( B ) Axial image.
Post-contrast CT puffed cheek technique facilitates better visualization of this right T1 buccal mucosa SCC. ( A ) Axial puffed cheek view shows the right buccal SCC ( red arrow ). ( B ) Coronal puffed cheek view shows the right buccal SCC ( red arrow ).
Post-contrast CT in soft tissue ( A ) and bone algorithm ( B ) shows right buccal SCC read as radiographic T4a due to suspicion of bone erosion ( red arrows ). Following surgery, the tumor was staged as pT1. Close inspection of repeat full puffed cheek in angled view in soft tissue ( C ) and bone algorithm ( D ) shows improved visualization of the primary tumor and adjacent bone ( red arrows ).
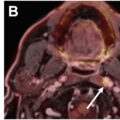
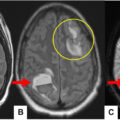
MR imaging offers improved delineation of tumor extent, better evaluation of bone marrow infiltration and more sensitive detection of perineural spread ( Fig. 10 A–D ). , Perineural spread occurs when tumors migrate from the primary site along the neural sheath, which can have significant consequences on staging, treatment strategies, and prognosis. , To evaluate perineural tumor spread, the imaging protocol should be optimized to evaluate the entire neural pathway from target organ to nucleus. Imaging features of perineural spread can be seen on CT, such as widening of the bony neural foramina; however, MR imaging is the optimal modality when perineural tumor involvement is suspected.