Perineural spread (PNS) is a clinically significant route of tumor extension in head and neck malignancies and is not uncommonly overlooked on imaging. Often clinically occult, PNS may first be suggested by radiologists, and its detection can have significant implications for prognosis and management. This article provides a comprehensive overview of PNS, including relevant cranial nerve anatomy, optimized imaging protocols, and characteristic radiologic features. Multiple illustrative cases are included to improve recognition and highlight the critical role of imaging in the early identification of this often occult disease process.
Key points
-
•
Perineural spread is a key pathway of tumor extension and affects staging, prognosis and management.
-
•
Radiologists play a critical role in suggesting PNS on imaging as it can be clinically occult.
-
•
Understanding relevant anatomy and characteristic imaging appearance is primordial.
Abbreviations
| ACC | adenoid cystic carcinoma |
| ADC | apparent diffusion coefficient |
| CECT | contrast-enhanced computed tomography |
| CSF | cerebrospinal fluid |
| CT | computed tomography |
| FDG | fluorodeoxyglucose |
| FR | foramen rotundum |
| GSPN | greater superficial petrosal nerve |
| HPV | human papillomavirus |
| IAC | internal auditory canal |
| IOF | inferior orbital fissure |
| NGF | nerve growth factor |
| PNI | perineural invasion |
| PNS | perineural spread |
| SCC | squamous cell carcinoma |
| T1w | T1-weighted |
| T2w | T2-weighted |
Introduction
Perineural spread (PNS) is a widely recognized and extensively described pattern of tumor spread, particularly in head and neck cancer. While perineural invasion (PNI) refers to microscopic tumor growth into the nerve, PNS describes tumor extension along the sheath of larger nerves and is typically seen on imaging.
PNS is generally associated with a poor prognosis and can occur independently of hematogenous or lymphatic dissemination. , Its prevalence varies according to tumor type and location. Neurotropic tumors with greater affinity for PNS include adenoid cystic carcinoma (ACC) of the salivary glands, squamous cell carcinoma (SCC), non-Hodgkin’s lymphoma, and melanoma. While ACC has the strongest association with PNS, it is most frequently seen in SCC because of its higher prevalence among head and neck malignancies. Some anatomic locations are particularly susceptible to PNS, whether they are the primary site of disease or secondarily involved. Primary sites most at risk for PNS include: the skin, parotid gland, nasopharynx, and hard palate. Other sites that carry a higher risk for PNS include the masticator space, pterygopalatine fossa, cavernous sinus, and Meckel’s cave. Furthermore, the most commonly involved nerves are the trigeminal and facial nerves.
Detecting PNS on imaging can be challenging, as findings are often subtle. It is, however, crucial to identify given its impact on treatment planning. PNS can render a resectable tumor unresectable and may require expanding the radiation field to include the affected nerve when radiation therapy is considered. Also, failure to recognize PNS can lead to disease progression due to suboptimal treatment.
Relevant anatomy and interconnections
PNS most commonly involves the trigeminal (CN V) and facial (CN VII) nerves. Important interconnections exist between these nerves, which are crucial to understand, as tumors can spread from a nerve to another along these interconnected pathways.
CN V1: The Ophthalmic Division
The cisternal portion of the trigeminal nerve originates from the lateral aspect of the mid pons and enters Meckel’s cave where its sensory fibers converge to form the trigeminal ganglion. Distal to the ganglion, the nerve gives rise to its 3 major divisions: ophthalmic (V1), maxillary (V2), and mandibular (V3) ( Fig. 1 ). The ophthalmic division then courses through the lateral aspect of the cavernous sinus and further divides into the nasociliary, frontal, and lacrimal branches prior to exiting the skull base through the superior orbital fissure. The ophthalmic nerve (CN V1) and its branches are best evaluated on coronal post-contrast T1-weighted (T1w) images through the cavernous sinus and orbits, respectively ( Fig. 2 A–H).
Illustration showing the trigeminal nerve divisions and selected sensory branches.
Axial T1w ( A , C , E ) and postcontrast T1wFS ( B , D , F ) images showing thickening and enhancement along the course of CNV1 with infiltration of the perineural fat within the orbit ( arrow , A and B ), superior orbital fissure ( arrow , C and D ), up to the cavernous sinus ( arrow , E and F ). Coronal pre ( G ) and post ( H ) contrast images showing thickening and enhancement of the left CNV1 in the superior extraconal region ( arrow ).
CN V2: The Maxillary Division
After originating from the trigeminal nerve within Meckel’s cave, the maxillary division courses along the lateral and inferior aspects of the cavernous sinus. It then exits the skull base through the foramen rotundum (FR), which serves as an entry point into the PPF, an “autonomic crossroads” and key pathway for PNS. The PPF communicates with the nasal cavity medially through the sphenopalatine foramen, with the infratemporal fossa laterally though the pterygomaxillary fissure, with the orbit superiorly through the inferior orbital fissure (IOF), with the palate inferiorly though the greater and lesser palatine foramina and with the middle cranial fossa posteriorly through the FR superiorly and the vidian canal inferiorly ( Fig. 3 A–F). The PPF serves as a conduit for PNS between the nerves coursing through these foramina ( Figs. 4 A–D and 5 A–E ).
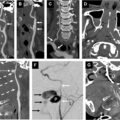
( A ) illustration showing sections through the PPF. ( B ) Axial noncontrast head CT through the foramen rotundum (FR) (corresponding to the red line in A ). ( C ) Lower axial CT through the vidian canal (corresponding to the light blue line in A ). ( D ) Coronal CT through both the FR and vidian canal (corresponding to dark blue line in A ). ( E ) Sagittal CT through the greater palatine canal (corresponding to green line in A ). ( F ) Axial CT through the greater and lesser palatine foramina. FR, foramen rotundum; GPC, greater palatine canal; GPF, greater palatine foramen; IOF, inferior orbital fissure; LPF, lesser palatine foramen; PMF/PPF, pterygomaxillary fissure/pterygopalatine fossa; SPF, sphenopalatine foramen; VC, vidian canal.
( A ) Axial CECT showing perineural spread of nasal SCC into the left greater than right infraorbital CNV2 ( white arrow ). ( B , C ) Sagittal CECT showing soft tissue thickening and enhancement within the infraorbital foramen ( arrows ) and inferior orbital fissure ( arrowhead ) on the right ( B ) and left ( C ) extending into the PPF ( asterisk ). ( D ) Illustration highlighting the likely involved segments and branches of the maxillary division of CN V2.
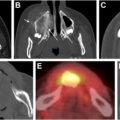
70-year-old man with adenoid cystic carcinoma of the right maxilla. ( A, B ) Two contiguous axial CECT show PNS with widening of the greater palatine foramen ( arrow ) and sclerosis of pterygoid plates. Axial T1wFS postcontrast ( C ) and axial T2w ( D ) show corresponding heterogeneously enhancing and ill-defined pterygoid plates. Arrowhead points to the contralateral normal pterygoid plates. ( E ) axial T1wFS postcontrast shows widening and enhancement of the right vidian canal ( short arrow ) likely involved by PNS.
Two branches of CN V2 are worth mentioning in the setting of PNS: the infraorbital nerve and the zygomatic nerve. Both originate from the maxillary division within the PPF; enter the orbit through the IOF; and course within the inferior extraconal space. The infraorbital nerve traverses the infraorbital canal and supplies sensory innervation to the upper lip, medial cheek, and lateral nose via its terminal branches. The zygomatic nerve divides into the zygomaticotemporal and zygomaticofacial branches, which exit through their respective foramina in the zygomatic bone and supply parasympathetic fibers to the lacrimal nerve, a branch of CN V1.
Communication with CN VII
Within the PPF, CNV2 transmits and receives parasympathetic nerve fibers through the pterygopalatine ganglion. In particular, it receives fibers from the Vidian nerve, which is a continuation of the greater superficial petrosal nerve (GSPN), a branch of CN VII, after merging with the deep petrosal nerve, a branch of the sympathetic plexus associated with the internal carotid artery ( Fig. 6 A–C).
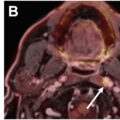
Buccal SCC with PNS along greater superficial petrosal nerve (GSPN). ( A ) Illustration shows GSPN ( purple ) connecting CNV2 and CN VII. ( B ) and ( C ) Axial T1wFS postcontrast showing nodular enhancement along the expected course of the GSPN ( arrow , B ) and in the meatal segment of the left facial nerve ( arrow , C ).
CN V3: The Mandibular Division
The mandibular division of the trigeminal nerve (CN V3) exits the skull base through the foramen ovale, bypassing the cavernous sinus, and enters the infratemporal fossa. There, it divides into an anterior and a posterior division. The anterior division, which is primarily motor, gives rise to the masseteric, lateral pterygoid, and deep temporal nerves, while also carrying the sensory buccal nerve. The posterior division is predominantly sensory and gives off the auriculotemporal, lingual, and inferior alveolar nerves, but also carries motor fibers.
CNV3 primarily supplies the masticator muscles, the mylohyoid muscles, anterior belly of the digastric, the tensor tympani, and tensor veli palatini muscles. It also provides sensory supply to the tongue, mucosal oral cavity, lower lip, chin, and lateral side of the face and scalp. Malignancies arising from these sites can potentially spread along the corresponding branches of the trigeminal nerve.
Communication with CN VII
The auriculotemporal nerve originates from CNV3 posteriorly as 2 distinct roots that ultimately converge medial and posterior to the neck of the mandibular bone. It then courses between the external acoustic meatus and the temporomandibular joint, pierces the capsule of the parotid gland cranially, and divides again into 2 branches—the auricular branch posteriorly and the temporal branch anteriorly—both of which communicate with the extratemporal segment of the facial nerve. Although the auriculotemporal nerve itself is not visible on imaging, its expected course should be closely followed, particularly along the posterior aspects of the mandibular body and neck ( Fig. 7 A, B).
Oral SCC with PNS along auriculotemporal nerve. Axial T1w ( A ) and postcontrast T1wFS ( B ) show enhancing nodular thickening along the expected course of the auriculotemporal nerve wrapping around the mandible ( arrow ).
The mandibular nerve and the facial nerve also communicate through the Chorda tympani nerve, which arises from the mastoid segment of the facial nerve and joins the lingual branch of the mandibular nerve just below the skull base.
CN VII: The Facial Nerve
The facial nerve originates from the pontomedullary junction laterally, courses through the cerebellopontine angle cistern and enters the internal auditory canal, running along its superior and anterior aspects. Distal to the meatal segment, the labyrinthine segment extends to the geniculate ganglion, where it gives rise to 3 branches: the GSPN, the external petrosal, and the lesser petrosal nerves. From the geniculate ganglion, the nerve continues as the tympanic segment, running up to the pyramidal eminence, and becomes the mastoid segment, which extends to the stylomastoid foramen. Three branches arise from the mastoid segment: the nerve to the stapedius muscle, the Chorda tympani, and Arnold’s nerve. The facial nerve then exits the skull through stylomastoid foramen, enters and supplies the parotid gland running between the superficial and deep lobes ( Fig. 8 A–D). Five branches emerge from this segment as it exists along the anterior margins of the parotid gland: the temporal, zygomatic, buccal, and marginal mandibular and cervical nerves.
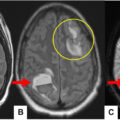
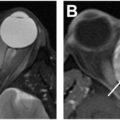
Malignant right parotid gland tumor with PNS along the facial nerve. Axial T2wFS ( A ), T1w ( B ), postcontrast T1wFS ( C ) and coronal postcontrast T1wFS ( D ) show marked thickening, T2w hyperintensity and enhancement from the mass to CNVII in the stylomastoid foramen ( arrow ) and mastoid portion ( arrowhead ).
Functionally, the facial nerve provides motor innervation to the muscles of facial expression, as well as the posterior belly of the digastric, stapedius, and stylohyoid muscles. It also provides sensory innervation to the auricle, external auditory canal, and mastoid region; taste fibers to the anterior two-thirds of the tongue; and parasympathetic innervation to the lacrimal gland (via the GSPN), submandibular and sublingual glands (via the Chorda tympani), and the parotid gland (via the lesser petrosal nerve).
Incidence, symptomatology, and prognosis
The incidence of PNS in head and neck cancers varies depending on the tumor type with a reported incidence up to 30% in mucosal SCC cases, and a lower incidence in cutaneous SCC. Site-specific differences also exist. For example, in a retrospective review study focusing on oral SCC specifically, PNI was identified in 17.4% of 430 patients. Another study focusing on laryngeal and hypopharyngeal SCC, found the incidence of PNI to be 33%. ACC has a higher propensity for PNS, but its lower prevalence as a histologic subtype makes SCC account for most cases of PNS. , Reported incidences of PNI in ACC are as high as 56%. ,
PNS has also been reported in melanoma, particularly in the desmoplastic subtype, though it remains relatively uncommon. While the progression of PNS in this subtype is slow, it is associated with a higher risk of intracranial extension. ,
The percentage of patients with PNS who develop symptoms also varies by tumor type and the affected cranial nerve. Approximately 30% to 40% of patients are asymptomatic, even when radiographic evidence of PNS is present. When symptoms do occur, they include pain, paresthesia, formication, weakness, or palsy. In the absence of a known primary, PNS can be misdiagnosed as a benign neuropathy. However, persistent facial nerve palsy or persistent trigeminal neuralgia should be considered red flags, warranting further evaluation, especially if conventional treatment has failed. Moreover, the involvement of multiple cranial nerves simultaneously may indicate extensive disease, such as leptomeningeal dissemination or contiguous spread, to a more central structure, such as the cavernous sinus.
The prognosis of patients with PNS in head and neck cancer is generally poor. The presence of PNS is associated with decreased survival and higher rates of local recurrence and metastasis. ,,
Known risk factors include: tumor location, size and stage, histologic differentiation, and post-treatment local recurrence. , Some studies also suggested that tobacco consumption and human papillomavirus (HPV) status may affect the likelihood of PNS. ,
Pathogenesis
The pathogenesis of PNI remains incompletely understood, but current evidence suggests it is multifactorial involving complex interactions between cancer cells and the neural microenvironment. Both malignant cells and nerves secrete molecular signals that modulate tumor behavior, promoting proliferation and inhibiting apoptosis. These molecular interactions can also enhance neural outgrowth toward the tumor, further facilitating PNI. Several factors are involved in head and neck malignancies including the brain-derived neurotrophic factor, nerve growth factor (NGF) and neural cell adhesion molecule, which are implicated in ACC and SCC. Additionally, the NGF receptor, also known as p75n, is also highly expressed in melanomas. Emerging studies have also highlighted the role of beta adrenergic and muscarinic receptors in perineural growth of certain malignancies, demonstrating that the inhibition of these receptors results in inhibition of tumor growth. Moreover, the role of Schwann cells has been increasingly recognized in tumorigenesis. Studies have shown a significantly higher concentration of dedifferentiated Schwann cells expressing glial fibrillary acidic protein surrounding tumor-associated nerves compared to normal nerve fibers. These findings not only confirmed the involvement of Schwann cells in PNI, but also identified the underlying cellular and molecular mechanisms.
Imaging protocols
MR imaging remains the gold standard imaging modality for cranial nerve evaluation. Dedicated protocols should be tailored to assess the nerve at the highest risk of PNS depending on the primary site of disease, and should include the entirety of the cranial nerve from the nucleus to the innervated end organ. Key sequences include: High resolution heavily T2-weighted (T2w) images and T1w non-FS images.
Heavily T2w sequences provide high-spatial resolution, which helps identify smaller cranial nerves. They also offer high soft tissue contrast allowing for better visualization of the dark cranial nerve against the background of bright cerebrospinal fluid (CSF), particularly in cisternal segments. ,,
These sequences should be appropriately selected: steady-state sequences, such as balanced fast field echo and constructive interference in steady state, provide excellent spatial resolution for central skull base anatomy but are prone to peripheral artifacts and should therefore be reserved for central structures (around the brainstem, for example). For more superficial nerves, other heavily T2w sequences, such as 3D DRIVE or 3D TSE, offer better visualization without peripheral distortion. Distal cranial nerve branches coursing through fat-containing soft tissue structures are best assessed on T1w-spin echo or fast-spin echo sequences, which provide better contrast resolution in these regions. , While post-contrast FS T1w images are helpful in assessing extracranial PNS, non-FS T1w images are preferred in intracranial PNS, as fat saturation can result in susceptibility artifact limiting cranial nerves evaluation at the skull base.
Other important imaging parameters used to optimize cranial nerve evaluation are: high magnetic field strength (1.5T or 3T), small field of view (i.e. 160– 180 mm), thin slices (3mm or less) and negligible gap (1 mm). Table 1 summarizes the protocol used at our institution for skull base imaging.
Table 1
Protocol used for imaging of CN V,VII,IX-XII on a 3T scanner
| Sequence | Coverage | FOV | Slice-Thickness/Gap | Base Resolution | TR | Sequence Type |
|---|---|---|---|---|---|---|
| SAG T1w IR | Whole Brain | 230 | 4/30% | 320 | 2000 | IR/TSE |
| AXIAL DWI | Cover from top of head through C2-C3 | 240 | 4/30% | 160 | >5000 | Resolve |
| AXIAL T2w FLAIR | Whole Brain | 230 | 4/30% | 320 | 9000 | IR/TSE |
| AX T2w DIXON | Top of frontal sinus to C2-C3 | 160 | 3.5/30% | 320 | 3000–5000 | TSE DIXON |
| AXIAL T1w DIXON | Top of frontal sinus to C2-C3 | 160 | 3.5/30% | 320 | 500–800 | TSE DIXON |
| Optional AX T2w 3D SPACE | Upper pons to C1 | 150 | 0.5/- | 320 | >1400 | SPACE |
| Optional T1w PERFUSION BRAIN | Cover tumor | 230 | 4/- | 192 | 4.91 | TWIST |
| +AX T1w DIXON THIN | Top of frontal sinus to C2-C3 | 180 | 3.5/30% | 320 | 600–800 | TSE DIXON |
| +COR T1w DIXON | Frontal sinus to 4th ventricle | 160 | 3/10% | 320 | 600–800 | TSE DIXON |
| +SAG 3D mpRAGE | Whole Brain | 250 | 0.9/- | 256 | 2300 | Turbo FLASH |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


