Head and neck cancers arise from an anatomically rich and complex region with multiple adjacent sites and subsites. The head and neck region’s intricate structures and complex anatomy make thorough physical examination challenging. Furthermore, direct scope assessment is primarily limited to mucosal surfaces and lesions. These limitations have led to an increased reliance on various imaging modalities. While squamous cell carcinoma is the most common malignant histology in the head and neck region, head and neck cancers encompass a variety of entities. This article focuses on sarcomas, cutaneous tumors, and extramedullary plasmacytoma of the head and neck.
Key points
-
•
Squamous cell carcinoma is the most common cancer in the head and neck region.
-
•
Rare sarcomas, rare cutaneous tumors, and extramedullary plasmacytoma can also occur in the head and neck.
-
•
The complex anatomy of the head and neck makes a thorough physical examination difficult.
-
•
Imaging plays a vital role in detecting and staging tumors, and in the assessment of treatment response.
Abbreviations
| AJCC | American Joint Committee on Cancer |
| BCC | basal cell carcinoma |
| CT | computed tomography |
| EMP | extramedullary plasmacytoma |
| MCC | Merkel cell carcinoma |
| MPNST | malignant peripheral nerve sheath tumor |
| NF1 | neurofibromatosis type 1 |
| SCC | squamous cell carcinoma |
Introduction
Head and neck cancers arise from an anatomically rich and complex region with multiple adjacent sites and subsites, with varying etiologic factors, diagnostic strategies, prognoses, and treatment approaches.
The head and neck region’s intricate structures and complex anatomy make thorough physical examination challenging. Furthermore, direct scope assessment is primarily limited to mucosal surfaces and lesions. These factors can lead to a delay in diagnosis of pathologic processes, in particular of deep neck lesions. These limitations have led to an increased reliance on various imaging modalities such as ultrasound, computed tomography (CT), MR imaging, and PET-CT to detect lesions, guide biopsy, aid in staging, direct treatment, assess treatment response, and determine prognosis.
While squamous cell carcinoma (SCC) is the most common malignant histology in the head and neck region, head and neck cancers encompass a variety of entities including rare histopathological entities. This article will focus on rare sarcomas, cutaneous tumors, and extramedullary plasmacytoma (EMP) of the head and neck.
Head and Neck Sarcomas
Sarcomas are malignant neoplasms that arise from mesodermal tissue. These rare tumors comprise less than 1% of solid malignancies throughout the body, with approximately 10% of sarcomas arising in the head and neck region.
According to the World Health Organization, sarcomas are subdivided into soft tissue sarcomas, bone sarcomas, and undifferentiated small round cell sarcomas.
Head and neck sarcomas typically arises from the more superficial soft tissues such as fat and muscles. This is unlike SCC, which are much more common and typically arises from the deeper aerodigestive tract. Another important distinguishing feature of head and neck sarcomas is the fact that lymphadenopathy is much less common in head and neck sarcomas in contrast to SCCs and lymphomas of the head and neck region.
The majority of soft tissue sarcomas of the head and neck is staged using a single American Joint Committee on Cancer (AJCC) TNM sarcoma staging system. T staging is based on size (T1-3) and invasion of adjacent structures (T4), with extent of invasion distinguishing stages T4a and T4b (see more details https://www.scribd.com/document/843123151/AJCC-Cancer-Staging-Manual-8ed-2017 ).
The N and M stages reflect lymph node and distant metastasis, respectively, and consist of N0 and M0 denoting the absence of regional lymph nodes or distant metastases. While N1 and M1 indicate the presence of regional lymph nodes or distant metastases, respectively.
Despite sarcoma’s rare involvement of the head and neck, multiple subtypes can involve the region with few demonstrating distinct imaging features (see more details https://www.scribd.com/document/843123151/AJCC-Cancer-Staging-Manual-8ed-2017 ). The following section will highlight some of these entities with emphasis on both clinical and imaging features.
Synovial sarcomas of the head and neck
Synovial sarcoma is a soft tissue sarcoma that presents as a slow-growing mass in teens or young adults. Head and neck involvement is exceedingly rare with only 5% to 7% of synovial sarcoma presenting in the head and neck region. In the head and neck, synovial sarcoma most commonly occurs in the hypopharynx, but other common locations include the paranasal sinuses, masticator space, and paravertebral space.
Imaging features
CT imaging of synovial sarcoma frequently demonstrates a solid mass with well-defined margins with heterogeneous enhancement after contrast administration. Calcifications can be seen in about 30% of cases.
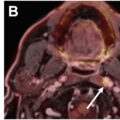
MR imaging of synovial sarcoma usually demonstrates a T1 isointense to slightly hyperintense mass compared to muscle. On T2, synovial sarcoma is hyperintense with a heterogeneous appearance. Post-contrast MR images frequently demonstrate a heterogeneously enhancing mass ( Fig. 1 A, B).
Synovial sarcoma. Patient presenting with right neck pain for more than 1 year. ( A ) MR imaging axial T2 demonstrates infiltrative heterogeneously hyperintense mass (relative to adjacent muscles) involving the right paraspinal musculature ( arrow ). ( B ) MR imaging axial fat saturated post-contrast image demonstrates an enhancing mass ( asterisk ) extending into the adjacent right C2-C3 neural foramen ( arrow ).
Diagnostic consideration and differential diagnosis
Imaging plays an essential role in detection of synovial sarcoma and staging the disease. However, given its nonspecific appearance overlapping with multiple other entities, biopsy remains essential for diagnosis.
Liposarcoma of the head and neck
Anatomic consideration and demographic factors
Liposarcoma represents up to 9% of head and neck sarcomas, with 81% arising in the subcutaneous fat, although they may be seen in and surrounding the aerodigestive tract. This tumor usually presents as a painless enlarging mass within the head and neck region. There are 5 subtypes, with 60% to 70% being the low-grade well-differentiated or myxoid subtypes. Rapid growth or change in imaging appearance can help suggest the dedifferentiated subtype.
Imaging features
On CT of the head and neck, liposarcoma typically presents as a large neck mass that can be trans-spatial with multiple components of varying attenuation reflecting its different contents. A key imaging feature that can help in establishing diagnosis is the presence of fat density suggestive of lipomatous content. The presence of thick septa or solid components can help suggest a more aggressive lipomatous lesion.
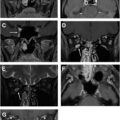
On MR imaging, liposarcoma presents with high signal intensity on T1-weighted images reflective of the fat content and heterogenous high signal intensity on T2-weighted images. Septations and solid components can demonstrate enhancement on post-contrast images and their presence can help in suggesting the diagnosis ( Fig. 2 A–C).
Liposarcoma. Patient presenting with a rapidly enlarging mass along the right posterior neck over the course of a few months. ( A ) Contrast enhanced neck CT, axial images demonstrate a heterogenous mass along the right posterior neck soft tissues that demonstrates fat density ( white arrow ), thick septations, and soft tissue nodules ( dashed arrows ). ( B ) MR imaging axial T1 sequence demonstrates hyperintensity reflective of fat density ( white arrow ) and intermediate signal reflective of soft tissue density ( dashed arrows ). ( C ) Axial fat saturated post-contrast image demonstrates enhancement of the soft tissue component ( dashed arrows ).
Aggressive liposarcomas, may appear as large, heterogeneous masses with variable attenuation, as they can have areas of fluid density, calcification, and fat density.
Diagnostic consideration and differential diagnosis
Well-differentiated liposarcomas can resemble the more common lipomas on imaging, as both may show thin septa and regions of increased signal intensity on T1 sequences reflective of fat content. Distinguishing features include thicker septate and solid enhancing soft tissue that, if present, can favor liposarcoma.
Liposarcomas can have a wide range of appearances, with both fat and soft tissue components (see Fig. 2 ). Less differentiated liposarcomas contain more soft tissue and less adipose tissue, making them more difficult to identify as fat-containing lesions which can lead to the lesions being mistaken as other types of sarcomas on imaging.
Leiomyosarcoma of the head and neck
Anatomic consideration and demographic factors
Leiomyosarcoma is a soft tissue tumor that arises from smooth muscles. These tumors are rare in the head and neck region and represents approximately 1% to 4% of all head and neck sarcomas with middle aged adults most commonly affected. Leiomyosarcoma of the head and neck is frequently described as intraoral (42%) with maxillary involvement, or extraoral (58%), which most frequently affects the thyroid gland.
Imaging features
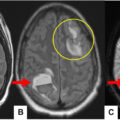
CT often exhibits leiomyosarcoma as a nonenhancing or faintly enhancing, heterogeneous mass with attenuation similar to muscle ( Fig. 3 A, B).
Leiomyosarcoma. Patient presenting with symptoms of nasal obstruction for few months. Patient has history of sinonasal mass 10 years prior, pathology unavailable. ( A ) Non contrast CT (NCCT) axial images of sinuses demonstrates an expansile mass obstructing the left nasal cavity ( arrows ) concerning for recurrence. ( B ) MR imaging axial fat saturated post contrast image demonstrates avid enhancement of the mass within the nasal cavity ( arrows ). At resection, pathology confirmed leiomyosarcoma.
On MR imaging, leiomyosarcoma typically demonstrates low-to-intermediate signal intensity on T1 sequences and high signal intensity on T2-weighted images. Peripheral enhancement can be present. Tumors generally demonstrate marked diffusion restriction.
Diagnostic consideration and differential diagnosis
The differential diagnosis includes pleomorphic undifferentiated sarcoma, fibrosarcoma, and desmoid tumor. Given the lack of specific imaging features, biopsy is needed for definitive diagnosis.
Ewing sarcoma of the head and neck
Anatomic consideration and demographic factors
Ewing sarcoma is a highly malignant tumor of bone and soft tissues that predominantly affects children and young adults with a predilection for the axial and appendicular skeleton. Ewing sarcoma of the head and neck is rare and accounts for less than 10% of Ewing sarcoma cases.
Ewing sarcoma of the head and neck region can occur in both skeletal and extra-skeletal forms, each with distinct radiological features. Skeletal disease most commonly involves the mandible which represents the most commonly affected facial bone. Extra-skeletal Ewing sarcoma is rarer in the head and neck, with few cases reported in the maxillofacial region and buccal mucosa. Extra-skeletal lesions may present as firm swelling, either with or without pain.
Imaging features
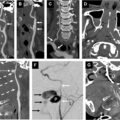
CT is excellent for depicting the aggressive osseous findings of skeletal Ewing sarcoma which include any or all of the following: bone destruction, moth-eaten or permeative changes, aggressive onion skin or spiculated periosteal reaction, and wide transitional zone of the lesion ( Fig. 4 A).
Sinonasal Ewing sarcoma. Patient presenting with symptoms of nasal obstruction. ( A ) CECT coronal images demonstrate a large obstructive mass involving the right sinonasal cavity with orbital involvement ( dashed arrow ). Note the ability of CT to detect the associated medial orbital wall spiculated periosteal reaction which can serve as a clue to the diagnosis ( white arrow ). ( B ) MR imaging coronal T2 better delineates the extent of nasal cavity involvement ( arrows ). ( C ) MR imaging coronal post-contrast images demonstrate enhancement of the lesion extending into the right orbit ( arrows ).
MR imaging is excellent for detection of extent of bone marrow involvement and is superior to CT for the delineation of soft tissue components. MR imaging typically shows hyperintensity of the involved bone marrow on fluid-sensitive sequences with loss of the normal marrow signal on T1. Soft tissue disease has variable signal intensity on MR imaging with low signal on multiple sequences attributed to bone/calcifications. The soft tissue component often demonstrates heterogenous T2 hyperintensity and solid or heterogenous enhancement ( Fig. 4 B, C). Ewing sarcoma frequently demonstrates diffusion restriction on the DWI sequence. ,
Bone scan may often demonstrate increased radiotracer uptake in bony primaries. FDG-PET/CT is frequently utilized for staging and evaluating treatment response as lesions are frequently FDG-avid and can be followed for treatment response on subsequent examinations.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


