Mandibular and maxillary lesions are common imaging findings, which pose a unique diagnostic challenge as dental pathology overlaps that of the remainder of the oral cavity. This review will guide radiologists in the interpretation of benign and malignant odontogenic and non odontogenic neoplasms.
Key points
-
•
Jaw lesion imaging characteristics can help identify benign versus malignant disease.
-
•
The location of a lesion with respect to the dentition is an important consideration.
-
•
Systemic diseases can affect the jaw.
Abbreviations
| AC | ameloblastic carcinoma |
| AF | ameloblastic fibroma |
| AFS | ameloblastic fibrosarcoma |
| AOT | adenomatoid odontogenic tumor |
| BOCs | botyroid odontogenic cysts |
| CCOC | clear cell odontogenic cyst |
| CEOT | calcifying epithelial odontogenic tumor |
| DCs | dentigerous cysts |
| GCOC | ghost cell odontogenic cyst |
| GOCs | glandular odontogenic cysts |
| LCH | langerhans cell histiocytosis |
| LPCs | lateral periodontal cysts |
| OKC | odontogenic keratocysts |
| OS | odontogenic sarcomas |
| POTs | primordial odontogenic tumors |
| RC | radicular cyst |
| SOC | sclerosing odontogenic carcinoma |
Introduction
Mandibular and maxillary lesions are common imaging findings, which pose a unique diagnostic challenge as dental pathology overlaps with that of the remainder of the oral cavity. Differentiating incidental lesions from those which cause significant morbidity and even mortality can be difficult. This article will provide a classification framework for jaw lesions and help the interpreting radiologist guide patient management. Identifying lesions that are of odontogenic origin based on lesion descriptors and location is a good first step in approaching the differential.
The main components of the teeth are enamel, dentin, pulp, and cementum, anchored to the alveolus by the periodontal ligament. Dental enamel is derived from the oral ectoderm during odontogenesis, formed by ameloblasts within the epithelium. The dentin and cementum, derived from the neural crest, are formed by odontoblasts and cementoblasts respectively. The more complex dental pulp and periodontal ligament are associated with odontoblasts, fibroblasts, osteoblasts, and endothelial cells. Both proliferation and inflammation of these dental components and the epithelial and mesenchymal cells that form them play a role in the formation of odontogenic lesions. The cystic, solid and/or nonmass-like sclerotic appearance of the lesions, their infiltrative, erosive and/or expansile nature, and location with respect to the erupted versus unerupted tooth can help narrow the odontogenic differential considerations.
Nonodontogenic maxillary and mandibular lesions have a broader differential, including mucosal space, salivary gland rest, and osseous and systemic pathologies. Systemic disease, the global bone marrow appearance, and involvement of adjacent structures such as the periosteum, mucosal space, hard palate, cranial nerve branches, and deep cervical soft tissues factor into the differential diagnosis of nonodontogenic lesions.
The location of mass-like lesion with respect to the adjacent dentition and alveolus is a critical factor. Like osseous lesions outside of the jaw, the zone of transition and ability to delineate the lesion from adjacent normal appearing structures can help identify lesion location. The more benign or chronic process have descriptors such as osseous remodeling, tooth displacement and chronic appearing periosteal new bone formation. In contrast, the inflammatory, infiltrative and/or malignant processes exhibit osseous erosion, soft tissue invasion and more aggressive periosteal reaction resulting in a sunburst or triangular configuration of new bone. Mass-like lesions can be described as cystic, solid or mixed, with or without peripheral versus central enhancement, internal mineralization, and/or fluid-fluid levels.
Using these descriptors and lesion location with respect to the dentition in combination with known systemic disease can significantly improve the ability to confidently narrow differential considerations before recommending tissue diagnosis.
Well circumscribed cystic lesions
Most jaw lesions will present as hypoattenuating-radiolucent lesions or cystic masses. The first step in formulating the differential diagnosis is to distinguish inflammatory lesions associated with the dentition from cystic masses in tooth bearing versus nontooth bearing areas of the alveolus. Hypoattenuating-radiolucent odontogenic lesions are most commonly inflammatory and the relationship of a cystic mass to the dentition is essential in differentiating among odontogenic cysts and neoplasms.
Apical rarefying osteitis, synonymous with apical periodontitis, appears as a circumscribed lytic area at the root with egress of inflammation from pulpal necrosis. Chronic Apical Rarefying Osteitis may develop an epithelial lining and form a cyst, called a Radicular Cyst (RC), the most common cystic odontogenic lesion. ,, RCs can expand or erode through the cortex when large, mimicking other cystic odontogenic neoplasms ( Fig. 1 A–C ).
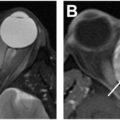
Radicular cyst (RC). Axial T2 space ( A ) and contrast enhanced fat saturated axial T1 ( B ) show a uniformly T2 hyperintense lesion with a thin enhancing rim ( arrows ). Coronal bone CT ( C ) shows the mass emanating from the root of the left maxillary lateral incisor with carious amputation of the crown ( arrow ).
Dentigerous Cysts (DCs), the most common noninflammatory odontogenic cyst, arise from fluid accumulation in the follicle surrounding an unerupted or impacted tooth. ,,, DCs are typically solitary and circumscribed, surrounding the crown of an unerupted or impacted tooth, most commonly involving the mandibular third molars ( Fig. 2 A, B ). The apex of the cyst will be at the cementoenamel junction (see Fig. 2 ). Large DCs will expand the alveolus, displace adjacent teeth, and envelop the involved tooth. The cyst wall is thin and corticated on computed tomography (CT), though chronic hydrostatic pressure or superimposed inflammation may result in wall thickening or dehiscence with mild peripheral enhancement. The nonenhancing central cystic contents will be hypoattenuating in the absence of proteinaceous debris or cholesterol granules, with a corresponding appearance on MR imaging ( Fig. 3 A–C ). Lack of diffusion restriction is important in differentiating DCs from other benign or malignant odontogenic and nonodontogenic lesions. The presence of multiple DCs is rare, typically syndromic, and can be associated with odontogenic keratocyst syndromes.
Dentigerous cyst (DC). Axial bone CT ( A ) shows a unicystic hypoattenuating expansile mass surrounding the right mandibular third molar. The intact cortex is remodeled ( long arrow ) with posterior displacement of the inferior alveolar neurovascular canal ( short arrow ). Coronal bone CT ( B ) shows that the cystic mass extends from the cementoenamel junction ( long arrows ) surrounding the crown.
Dentigerous cyst (DC). Sagittal T2 space ( A ) shows a uniformly T2 hyperintense mass extending from around the cementoenamel junction of an impacted molar (arrows). Contrast enhanced axial T1 ( B ) demonstrates a uniformly thin enhancing cyst wall ( arrow ). Axial apparent diffusion coefficient (ADC) ( C ) shows no restricted diffusion ( arrow ).
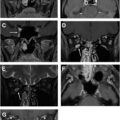
Tooth involvement is one of the key features which distinguishes a large expansile DC from an OKC. OKCs can displace, partially resorb, or engulf a tooth, although the cyst wall is not directly associated with the cementoenamel junction. As opposed to the follicle of an unerupted tooth, odontogenic keratocysts (OKCs) develop from the dental lamina and are most common in the posterior mandible (up to 80%) of young males in their second-third decade of life. OKC typically presents as an expansile unilocular cystic lesion with well-defined sclerotic borders that can become scalloped as the lesion grows , ( Fig. 4 A–C ). The mandibular ramus is often involved in larger lesions, necessitating scrutinous evaluation for an associated pathologic fracture. It is important to assess for extraosseous extension as these lesions are notoriously difficult to surgically resect from soft tissue ( Fig. 5 A ). OKCs can have a heterogenous central appearance on precontrast MR imaging secondary to the presence of parakeratin, although they should only demonstrate peripheral enhancement ( Fig. 5 B, C). Small lesions are often found incidentally. Pain and trismus can develop as the lesion grows, with associated cellulitis and drainage in the setting of superinfection. OKCs can grow rapidly and have a high recurrence rate after surgical treatment. The amount of enhancement can increase in the setting of recurrence. OKCs can also be multilocular, septate, and multifocal. More complex multilocular and septate OKCs can be difficult to confidently delineate from an ameloblastoma, for which postcontrast MR imaging or CT imaging can be helpful to identify central nodular enhancement of ameloblastoma. Multifocal disease should raise suspicion for syndromic etiologies such as basal cell nevus syndrome ( Fig. 6 A–C ), Gardener’s syndrome, clediocranial dysplasia or mucopolysacchroidosis VI. Multifocal expansile lucent jaw lesions can also be seen in the setting of cherubism, with improvement as patients grow beyond puberty.
Dentigerous cyst (DC) versus odontogenic keratocyst (OKC). Axial bone CT ( A ) shows a unicystic expansile mass that appears to be arising from around the crown of the unerupted right mandibular third molar ( arrows ). The differential diagnosis starts with DC. Axial unenhanced CT ( B ) in the same patient shows a geographic area of increased attenuation prompting consideration for OKC and ameloblastoma. Coronal bone CT ( C ) demonstrates extension of the lesion along the long axis of the mandibular ramus with nonuniform cortical thinning ( arrows ). While not pathognomonic, this occurs more commonly with OKCs; pathology confirmed OKC.
Odontogenic keratocyst (OKC). Axial enhanced CT in Patient #1 ( A ) shows a non-enhancing marginated cystic mass in the left mandibular ramus ( long arrow ). Focal dehiscence (short arrow) permits extraosseous extension into the masseter muscle ( arrowheads ). Axial T1 in Patient #2 ( B ) shows hypointense mass expanding the right mandibular ramus with central T1 hyperintensity (arrows) of the characteristic parakeratin seen in OKCs. ( C ) Axial T2 ( C ) shows a predominately T2 hyperintense cystic lesion ( white arrow ) with centrally hypointense parakeratin.
Basal cell nevus syndrome. Axial bone CT ( A ) shows a unicystic expansile and lobulated eccentric mass ( arrows ) involving the tooth bearing left mandibular alveolus and molar. Ameloblastoma and OKC are considered. Axial bone CT ( B ) reveals an additional unicystic mass in the right mandibular ramus ( arrows ). The presence of multiple odontogenic cysts narrows the differential to OKCs or DCs associated with a syndrome. Photograph ( C ) shows a basal carcinoma ( arrow ) in this patient with multifocal OKCs in the setting of basal cell nevus syndrome.
An ameloblastoma is a benign odontogenic neoplasm of epithelial origin, which occurs in the tooth bearing portions of the mandible and maxilla. Ameloblastomas can arise from the epithelium of the tooth germ, enamel organ or odontogenic cyst lining, and occur in the posterior mandible approximately 80% of the time. , In contrast to OKCs, ameloblastomas typically have a more complex appearance, presenting as a cystic and solid expansile mass with scalloped margins and enhancing soft tissue components ( Figs. 7 A–G and 8 A, B ). , They can be unicystic or multicystic, with the number of cystic components increasing with the age at presentation. MR imaging can be useful to define the soft tissue components and their margins, with specific attention to the mandibular canal, adjacent deep spaces of the suprahyoid neck, and, in the case of maxillary lesions, the maxillary sinuses, nasal cavity, and orbit. Ameloblastomas can be divided into histopathologic subtypes, with the follicular subtype having the highest recurrence rate , and mixed acanthomatous or desmoplastic lesions demonstrating aggressive local invasion due to matrix metalloproteinases ( Fig. 9 A–E ). En bloc surgical resection with osseous margins is the treatment of choice, demonstrating a significantly improved recurrence rate compared to more conservative management often reserved for younger patients and unicentric disease.
Unicystic ameloblastoma. Axial bone CT ( A ) in Patient #1 shows a classic Unicystic ameloblastoma as a lobulated cystic mass expanding the right mandibular body ( arrows ). Coronal bone CT ( B ) shows that the mass involves the right mandibular second molar with the center (★) and the vector of extension ( dashed arrows ) suggesting the apex is not at the cementoenamel junction (DC less likely). Axial unenhanced CT ( C ) demonstrates slight central hypoattenuation to muscle. Axial bone CT ( D ) in Patient #2 shows cystic lesion in the right mandibular ramus with thickened osseous scalloping or septation ( white arrow ) thatoccurs more frequently with ameloblastomas than OKCs or DCS. Sagittal bone CT ( E ) shows the lesion with mildly scalloped margins ( white arrows ) pushing up against the crown of the molar tooth crossing the cementoenamel junction ( black arrows ). Enhanced axial ( F ) and sagittal ( G ) CT in Patient #3 show a unicystic ameloblastoma in the mandibular symphysis with an eccentric focus on nodular enhancing soft tissue mural nodule ( arrows ), which can indicate a higher risk of recurrence and extraosseous extension.
Multicystic (conventional) ameloblastoma. Axial bone CT ( A ) shows the classic Multicystic ameloblastoma in the left mandible as an expansile lobulated cystic mass with coarse septations ( arrows ) giving rise to the description of bubbly in the literature. Axial unenhanced CT ( B ) shows the heterogeneous hyperattenuation and hypoattenuation of mixed solid ( long arrow ) and cystic ( short arrow ) components, reflecting the tumor islands and cysts characteristic of multicystic Ameloblastomas.
Acanthomatous ameloblastoma subtype. Axial bone CT ( A ) in Patient #1 shows a cystic expansile right parasymphaseal mandibular mass associated with an unerupted premolar tooth. The coarse septations ( long arrow ) and loculated appearance ( short arrow ) suggest a multicystic ameloblastoma. Axial unnhanced CT ( B ) shows the soft tissue component of the mass to be hyperdense ( arrow ). This was a mixed acanthomatous, desmoplastic ameloblastoma; the desmoplastic components containing significant fibrous tissue. Axial T1 ( C ) in Patient #2 shows a T1 hypointense mass infiltrating from the left maxillary alveolus through the pterygoid plates (short arrow) and into the medial ptyergoid muscle ( long arrow ). Fat saturated axial T2 ( D ) shows the mass to be largely T2 intermediate to hypointense with focal areas of T2 hyperintensity ( arrow ) and axial ADC ( E ) shows restricted diffusion ( arrows ), compatible with high cellularity. The infiltrative nature of this mass and high cellularity should prompt consideration for ameloblastic carcinoma, or other odontogenic carcinomas.
Less common cystic appearing odontogenic lesions include lateral periodontal cysts (LPCs), botyroid odontogenic cysts (BOCs), glandular odontogenic cysts (GOCs), and primordial odontogenic tumors (POTs). LPCs are noninflammatory developmental cysts typically measuring less than 1 cm along the lateral margin of a vital tooth root. LPCs often present incidentally as thin walled hypoattenuating lesions within the premolar mandible of adults in their fifth-seventh decades. , While the morphology is like that of dentigerous and gingival cysts, LPCs are intraosseous and associated with erupted teeth along the periodontal ligament space. BOCs are noninflammatory developmental cysts that are also most common in the premolar mandible; some believe they may arise from or are subsets of LPCs. In contrast to LPCs, BOCs can be multiloculated and tend to be larger at presentation, measuring up to 4.5 cm with mandibular expansion, pain, and possibly paresthesia. GOCs are developmental cysts that present in the fourth-fifth decade and are most common in the anterior mandible near or crossing the symphysis. , GOCs can be unilocular or multilocular and demonstrate slow growth over time but are locally aggressive with a propensity to recur, especially those treated with curettage or enucleation, versus resection with reconstruction. While the radiographic features can overlap ( Fig. 10 A, B ), GOCs can be differentiated from LPCs, BOCs, and Ameloblastomas histologically, demonstrating cilia, ducts, and mucous cells, true to their suspected salivary origin. , POTs also have a well-circumscribed lucent radiographic appearance despite central fibromyxoid tissue, which sets them apart from the fibrous tissue of ameloblastoma. POTs typically present in the first or second decade of life along the crown of an unerupted posterior tooth, often with tooth displacement and root resorption.
Glandular ondontogenic cyst. Axial bone CT ( A ) shows an expansile cystic left mandibular mass with thinned but relatively straight cortical margins ( white arrows ): consider OKC or Ameloblastoma. Axial enhanced CT ( B ) shows a central soft tissue mass of moderate increased attenuation and patchy areas of enhancement ( black arrows ): differential diagnosis is ameloblastoma.
Osteolytic, erosive, and infiltrative cystic lesions
Osteoradionecrosis and medication related osteonecrosis can result in trabecular irregularity with mixed lytic and sclerotic changes, cortical irregularity, sequestrum, and bone exposure. A history of radiation and offending medical therapy such as bisphosphonates, bevacizumab, and tyrosine kinase inhibitors are key to making the diagnosis. The mandible is more prone to osteonecrosis. Superimposed infection and subsequent osteomyelitis are more common in osteoradionecrosis. Cellulitis, abscesses, and draining sinus tracts can develop in the setting of osteomyelitis. Careful inspection for solid enhancement suggestive of recurrent disease is important in the setting of prior oral cavity-directed radiation therapy.
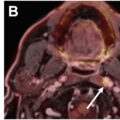
Langerhans cell histiocytosis (LCH) can also result in an osteolytic appearance of the jaw and can be molecularly classified as an inflammatory neoplasm. Imaging characteristics range from benign to aggressive, including ill-defined infiltrative borders with cortical destruction, periosteal new bone formation, sclerosis, soft tissue inflammation and lymph node involvement ( Fig. 11 A, B ). Symptoms include swelling, pain, bleeding with gingival ulceration, floating teeth, and pathologic fractures. Age at presentation, lack of infectious markers, and additional systemic lesions can be helpful to imply the diagnosis and prompt biopsy to exclude malignancy. Additional mandibular and maxillary neoplasms include those derived from salivary gland rests, the adjacent oral cavity, systemic disease and malignant transformation or variants of odontogenic lesions.