Best radiographic alternative to optical colonoscopy
Proper technique critical, including utilization of colon cleansing agent, stool “tagging” agent, electronic CO₂ insufflator, and separate supine and prone acquisitions
Polyps appear as small or large, sessile or pedunculated, lesions extending from colon wall
Polyps measuring ≤ 5 mm generally not reported
Polyps measuring ≥ 1 cm referred for polypectomy
• Air- (double) contrast barium enema
Sessile polyps
– Dependent wall: Radiolucent filling defect
– Nondependent wall: Ring shadow with barium-coated white rim
– Bowler hat sign: Brim and dome of hat represents base and head of polyp, with dome of hat pointing towards lumen of bowel (en face view)
Pedunculated polyps
– Mexican hat sign: Pair of concentric rings with outer and inner rings representing head and stalk of polyp
“Carpet” lesion: Tiny, coalescent nodules and plaques create a finely nodular or reticular pattern
PATHOLOGY
• Neoplastic polyps: Adenomatous (tubular, tubulovillous, and villous)
• Nonneoplastic polyps: Hyperplastic, hamartomatous, and inflammatory
• All adenomatous polyps contain foci of dysplasia and represent potential precursors to colon carcinoma
CLINICAL ISSUES
• Any polyp ≥ 1 cm on barium enema or CT colonography should undergo colonoscopic polypectomy
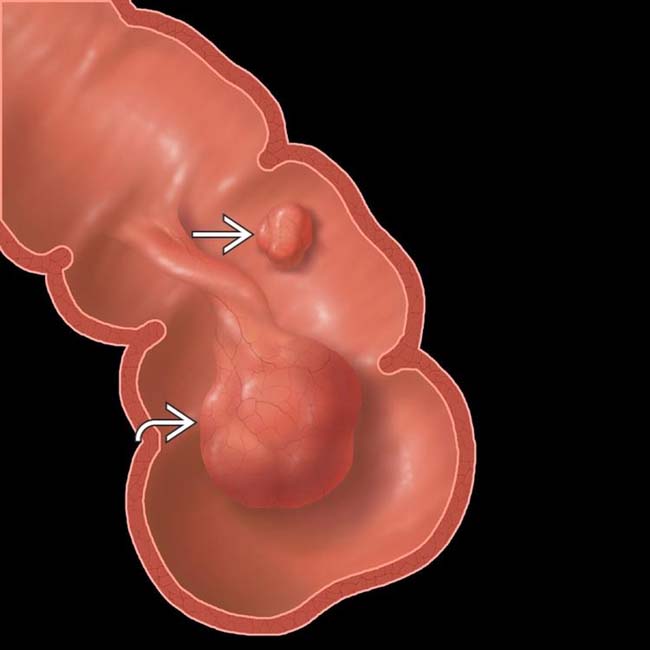
(Left) Graphic shows a tubulovillous adenoma on a long stalk and a small sessile polyp .
(Right) Single-contrast barium enema demonstrates a tubulovillous adenoma with a large head and a long stalk . A small sessile polyp is also seen.
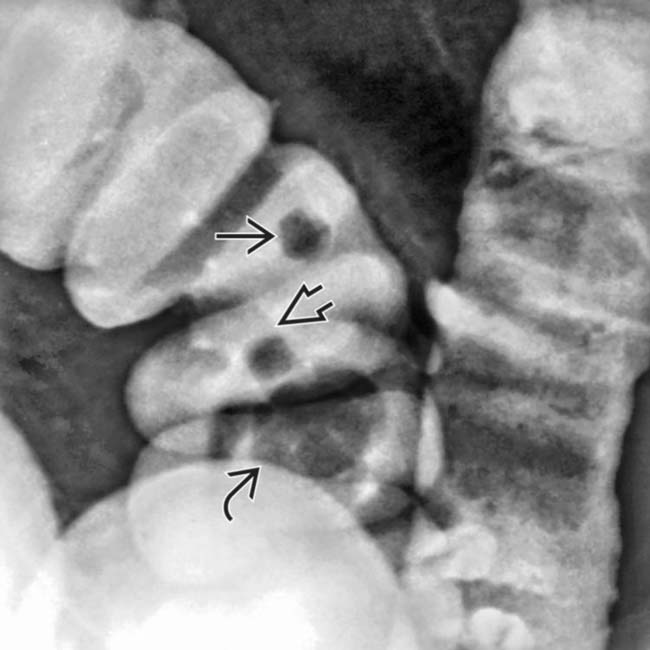
(Left) Air-contrast barium enema shows a large sessile polyp in the cecum, having the typical appearance of a villous adenoma, with cauliflower-like surface irregularity.
(Right) Air-contrast barium enema shows a small polyp on a short stalk . The outer rim of the “Mexican hat” is the head of the polyp, while the inner ring is the stalk.
TERMINOLOGY
Definitions
• Focal, space-occupying masses that arise from colonic mucosa and protrude into colonic lumen
IMAGING
General Features
• Best diagnostic clue
Smooth-surfaced intraluminal small mass on CT colonoscopy or barium enema
Sessile polyps: Broad base with little or no stalk
Pedunculated polyps: Arise from narrow stalk
• General features
2 types of colon polyps
– Neoplastic: Adenomatous (tubular, tubulovillous, and villous)
– Nonneoplastic: Hyperplastic, hamartomatous, and inflammatory
CT Findings
• CT “virtual” colonography
Proven superior to barium enema and now considered primary radiographic alternative to optical colonoscopy
– Advantages relative to optical colonoscopy: Shorter procedural time, ↓ risk to patient, and no IV sedation
– Technique primarily validated by national CT colonography trial conducted by ACRIN, which showed sensitivity of 90% and specificity of 86%
– Polyps ≥ 10 mm: Sensitivity of 90% per patient, 84% per polyp
– Detection of small polyps (< 1 cm) much less reliable
– Sensitivity for colorectal cancers is excellent (∼ 95%)
– Results vary based on reader experience, skill of interpretation, and technique used
Technique considerations
– Optimally performed after administration of colon cleansing agent (using either a “wet” or “dry” laxative preparation) and stool “tagging” agent
Tagging agents cause fecal residue to appear radio-opaque and easier to distinguish from polyps
“Dry” cathartics (i.e., magnesium citrate or sodium phosphate) preferred as they induce less fluid in colon compared to “wet” cathartics (i.e., polyethylene glycol)
Clear liquid diet (no solids) day prior to scan
– Colon insufflated with CO₂ using electronic insufflator to 25 mm Hg
– Separate supine and prone acquisitions allow differentiation of stool from polyps, better distension of some parts of colon, and redistribute fluid and fecal material (allowing better evaluation of entire mucosa)
Images best acquired in end expiration to minimize mass effect by lungs upon transverse colon
Additional left or right decubitus positioning may be necessary if portions of colon are not distended
– Study should be performed using low radiation dose technique
Interpretation
– Polyps appear as small or large, sessile or pedunculated, lesions extending from colon wall
– Images reviewed in 2D (axial data set) or 3D (endoluminal 3D reconstructions)
– Computer aided detection (CAD) systems may serve as diagnostic adjunct to routine image review
– As with barium enema, “flat” or “carpet” lesions can be challenging to detect on CT colonography
– Polyps measuring ≤ 5 mm generally not reported due to low specificity and low risk of malignancy
– Polyps measuring ≥ 1 cm referred for polypectomy
– Management of 6-9 mm polyps debatable and can be managed with either CT surveillance or polypectomy
Management debatable given that 6-9 mm polyps have incidence of malignancy as low as 0.1%
Reporting system (C-RADS)
– Colorectal findings (C0-C4)
C0: Inadequate study
C1: Normal or benign lesion (no polyps ≥ 6 mm)
C2: Intermediate polyp (polyps 6-9 mm)
C3: Possible advanced adenoma (polyps ≥ 10 mm)
C4: Possible malignant colorectal mass (lesion extends beyond lumen, extracolonic invasion)
– Extracolonic findings (E0-E4)
E0: Study compromised by artifact
E1: Normal extracolonic findings
E2: Clinically unimportant finding
E3: Likely unimportant but incompletely characterized
E4: Potentially important extracolonic finding
Radiographic Findings
• Air- (double) contrast barium enema (BE)
Limited in terms of sensitivity, with miss rates as high as 17% (up to 10% miss rate for polyps > 1 cm)
– Limited in areas of colonic redundancy or overlap, including rectosigmoid and hepatic/splenic flexures
Sessile polyps
– Dependent wall: Radiolucent filling defect
– Nondependent wall: Ring shadow with barium-coated white rim
– Bowler hat sign: Brim and dome of hat represent base and head of polyp, with dome of hat pointing towards lumen of bowel (en face view)
Pedunculated polyps
– Mexican hat sign: Pair of concentric rings with outer and inner rings representing head and stalk of polyp
Tubular adenomatous polyps
– Small in size and often pedunculated with only minor degree of villous changes
Tubulovillous adenomatous polyps
– Medium-sized, sessile polyps with fine nodular or reticular surface pattern and filling of barium within interstices of adenoma
Villous adenomatous polyps
– Larger, sessile polyps with barium trapped between frond-like projections, resulting in granular or reticular pattern
– ↑ lobulation, reticulation, or granulation in polyp usually associated with greater villous component
Only gold members can continue reading. Log In or Register to continue
 Proper technique critical, including utilization of colon cleansing agent, stool “tagging” agent, electronic CO₂ insufflator, and separate supine and prone acquisitions
Proper technique critical, including utilization of colon cleansing agent, stool “tagging” agent, electronic CO₂ insufflator, and separate supine and prone acquisitions





 on a long stalk and a small sessile polyp
on a long stalk and a small sessile polyp  .
.
 and a long stalk
and a long stalk  . A small sessile polyp
. A small sessile polyp  is also seen.
is also seen.
 in the cecum, having the typical appearance of a villous adenoma, with cauliflower-like surface irregularity.
in the cecum, having the typical appearance of a villous adenoma, with cauliflower-like surface irregularity.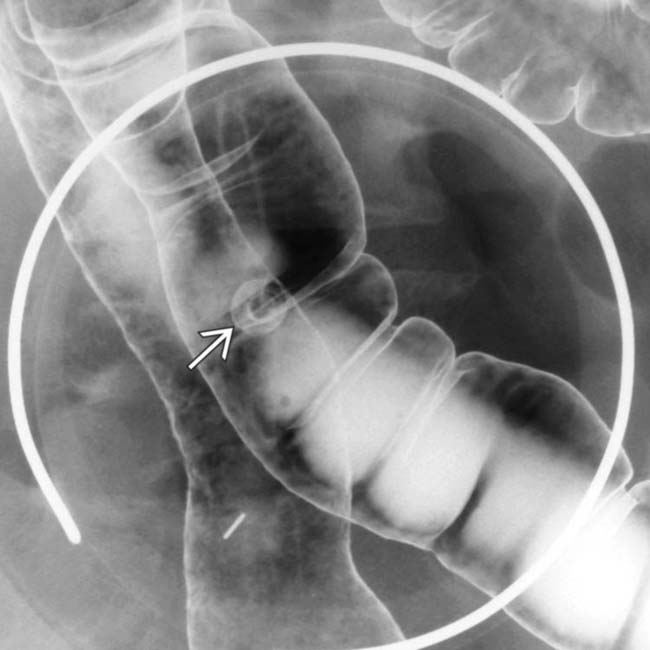
 . The outer rim of the “Mexican hat” is the head of the polyp, while the inner ring is the stalk.
. The outer rim of the “Mexican hat” is the head of the polyp, while the inner ring is the stalk.




 Proven superior to barium enema and now considered primary radiographic alternative to optical colonoscopy
Proven superior to barium enema and now considered primary radiographic alternative to optical colonoscopy Technique considerations
Technique considerations “Dry” cathartics (i.e., magnesium citrate or sodium phosphate) preferred as they induce less fluid in colon compared to “wet” cathartics (i.e., polyethylene glycol)
“Dry” cathartics (i.e., magnesium citrate or sodium phosphate) preferred as they induce less fluid in colon compared to “wet” cathartics (i.e., polyethylene glycol)
















 Limited in terms of sensitivity, with miss rates as high as 17% (up to 10% miss rate for polyps > 1 cm)
Limited in terms of sensitivity, with miss rates as high as 17% (up to 10% miss rate for polyps > 1 cm) Villous adenomatous polyps
Villous adenomatous polyps









