Chapter 122 At birth, the adrenal glands are relatively large because of the presence of the fetal adrenal cortex, which accounts for about 80% of the gland.1 Because of this, both adrenals are easily visualized by using ultrasonography in the neonate (Fig. 122-1). Figure 122-1 A longitudinal sonogram of a normal adrenal (arrows) in a 1-day-old newborn. On ultrasonography, the normal adrenal gland has a central hyperechoic stripe surrounded by a hypoechoic rim. The hypoechoic rim represents the fetal and the peripheral definitive cortex (see Fig. 122-1). The central hyperechoic stripe includes the medulla, the central veins of the adrenal, connective tissue, and probably also part of the fetal cortex.2 The surface of the adrenals is smooth or only slightly undulating (see Fig. 122-1). The easiest and most useful measurement of the adrenal is the limb width, which should normally be less than 4 mm.3 Overview and Imaging: A straight or discoid shape of the adrenal gland is seen on ultrasonography in association with certain congenital anomalies of the ipsilateral kidney, in which the kidney either is absent from its normal position in the renal fossa or is extremely small as a result of antenatal damage and dysplasia.4 The adrenal gland otherwise develops normally but assumes a flattened, discoid shape (Fig. 122-2). On ultrasonography, the adrenal retains its normal pattern of echogenicity. Straight adrenals are longer than otherwise normal glands, and they tend to be slightly thicker. Figure 122-2 A longitudinal sonogram of the right adrenal gland shows a straight adrenal (arrows) in a patient with right renal agenesis. Overview and Imaging: Horseshoe adrenal is a rare congenital anomaly, in which the right and left adrenal glands are fused. It is often associated with other anomalies of the kidneys and the central nervous system, asplenia with visceral heterotaxy, and other anomalies.5 A horseshoe adrenal appears on ultrasonography as a band of normal adrenal tissue crossing the midline in the upper abdomen above the kidneys (e-Fig. 122-3). The adrenal maintains normal echogenicity. The isthmus of the horseshoe adrenal usually passes behind the aorta, but in asplenia, it usually passes in front of the aorta.5 e-Figure 122-3 A transverse sonogram of the upper abdomen shows a horseshoe adrenal (arrows) in a patient with visceral heterotaxy (asplenia). Overview and Imaging: Adrenal congestion may occur in perinatal asphyxia or stress, but the mechanism for this is not clearly understood. On ultrasonography, the glands appear markedly enlarged but maintain their general overall shape and smooth surface (Fig. 122-4). This usually occurs bilaterally but may be seen unilaterally or focally within one gland.2 Loss of the normal central echogenic stripe occurs, and the fetal cortex may become a broad band of slightly increased echogenicity. A very thin peripheral anechoic rim that represents the definitive cortex may be present. Follow-up ultrasonography may show development of focal hypoechoic areas that represent focal hemorrhages or infarction.2 The changes may be reversible and the sonographic pattern may return to that of normal adrenal glands in patients who survive. Figure 122-4 Adrenal congestion in an 8-day-old full-term boy who developed necrotizing enterocolitis, cardiovascular collapse, and multiorgan failure. Overview: Congenital adrenal hyperplasia (CAH) refers to a group of autosomal recessive disorders, in which an enzymatic defect occurs in the pathway for cortisol biosynthesis in the adrenal cortex. The most common defect is a deficiency of the enzyme 21-hydroxylase, which affects females much more commonly than males.3 This leads to ambiguous sexual development in newborn girls or salt-losing crisis in newborns of either sex. The diagnosis of CAH is confirmed by the presence of elevated serum 17-hydroxyprogesterone (17-OHP). In addition, in female neonates with genital ambiguity, normal internal genitalia are seen on pelvic ultrasonography, and a normal (46, XX) karyotype. The 17-OHP level is diagnostic only when measured after the third day of life because a relatively high level is present in the immediate neonatal period in a normal newborn. Furthermore, 17-OHP assays may not be easily available. These delays, although relatively short, may contribute to the diagnostic dilemma and heighten parental anxiety. Therefore, ultrasonography in the immediate neonatal period may play a role as some specific signs of CAH are seen on ultrasonography.3
Congenital and Neonatal Conditions
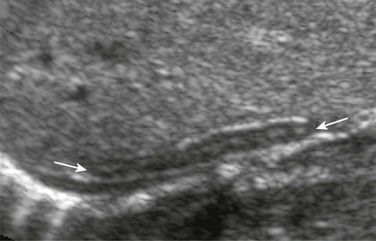
Normal Adrenal

The central hyperechoic stripe represents the central veins, connective tissue, medullary tissue, and congested sinusoids of the inner part of the fetal cortex. The surrounding hypoechoic zone represents the less congested outer part of the fetal cortex and the thin peripheral definitive cortex. The surface of the gland is smooth.
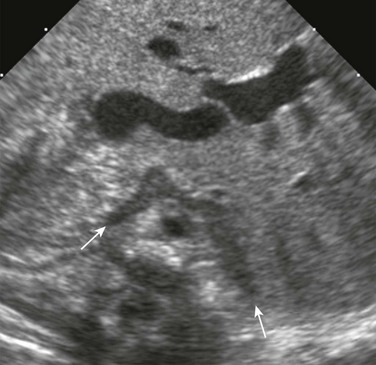
Abnormalities of Shape and Size
The adrenal gland is straight and lacks the angulation and shapes illustrated in Figure 122-1. The central hyperechoic stripe, surrounding hypoechoic zone, and smooth surface are preserved.
Horseshoe Adrenal
The adrenals are fused across the midline, giving a horseshoe shape. The central echogenic stripe and surrounding hypoechoic zone and smooth surface are maintained. The gland lies anterior to the aorta, which is to the right of the midline, and behind the inferior vena cava, which is to the left. (Courtesy Dr. Ulrich Willi, Kinderspital, Zürich, Switzerland.)
Adrenal Congestion
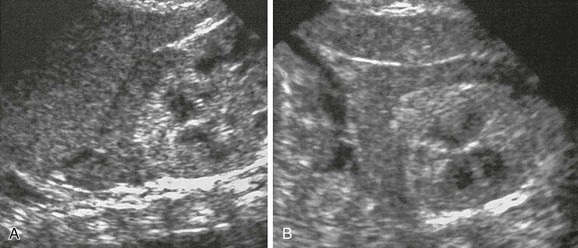
Longitudinal (A) and transverse (B) sonograms reveal marked enlargement of the left adrenal, which, although has retained its normal shape and smooth surface, shows loss of the normal central echogenic stripe. The gland has a more homogeneous low-level echogenicity, and in parts, a peripheral anechoic thin rim is seen. A postmortem histologic examination revealed congestion of the fetal cortex. The peripheral thin rim represents the peripheral definitive cortex.
Congenital Adrenal Hyperplasia








