Diagnostic Techniques
Thomas H. Berquist
Douglas S. Fenton
J. Mark McKinney
General concepts for diagnostic imaging techniques will be discussed in this chapter to avoid redundancy in subsequent chapters. Appropriate use of imaging techniques is essential for diagnosis, treatment decisions, and cost containment in today’s medical environment.
Routine Radiography
Today, routine radiography continues to be the most appropriate screening technique for musculoskeletal disorders. Appropriate evaluation of routine radiographs results in diagnosis or selection of the next most appropriate imaging procedure. Specifically, routine radiographs are essential for proper interpretation of magnetic resonance (MR) images.
Screen-film radiography is being replaced by computed radiography at many institutions. Regardless of the system used, it is essential to ensure proper patient positioning and chronologic labeling of images.
Multiple views (2–4) are required for minimal evaluation of osseous and articular anatomy. Specific views will be discussed in subsequent anatomic chapters. In some cases, fluoroscopically positioned spot views are useful to optimize positioning and reduce bony overlap. This approach is especially useful in the foot and wrist. This technique also is appropriate to evaluate interfaces of arthroplasties and metal fixation devices. Fluoroscopic positioning is particularly useful in the shoulder and knee. Stress views can be obtained using fluoroscopic guidance. Stress radiographs are especially useful in the ankle, elbow, knee, and wrist.
Suggested Reading
Bender CE, Berquist TH, Stears JG, et al. Diagnostic techniques. In: Berquist TH, ed. Imaging of orthopedic trauma, 2nd ed. New York: Raven Press; 1992:1–37.
Ultrasound
The term “ultrasound” refers to mechanical vibrations whose frequencies are above human detection. Ultrasound imaging uses frequencies from 2 to 12 MHz. Most musculoskeletal structures examined are superficial, requiring a 7- to 12-MHz transducer. Doppler ultrasound for peripheral vascular disease is approximately 8 MHz.
Musculoskeletal applications for ultrasound have expanded considerably in recent years. The joints, soft tissues, and vascular structures are particularly suited to ultrasound examination. Evaluation of cortical and trabecular bone now is feasible and permits examination of the calcaneus for osteoporosis.
Because of its low cost and availability, ultrasound now is being used more frequently to evaluate various conditions, as listed in Table 1-1.
TABLE 1-1 INDICATIONS FOR MUSCULOSKELETAL ULTRASOUND | |
|---|---|
|
Suggested Reading
Jacobson JA, Van Holsbeek MT. Musculoskeletal ultrasonography. Orthop Clin North Am 1998;29:135–167.
Lin J, Fassell DP, Jacobson JA, et al. An illustrated tutorial of musculoskeletal ultrasound. Part I, introduction and general principles. AJR Am J Roentgenol 2000;175:637–645.
Radionuclide Imaging
Multiple agents are available for bone imaging. The agents selected and imaging techniques used vary with the clinical indication for examination. Radiopharmaceuticals may be used alone or in combination.
Bone Scans
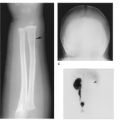
Patients are injected intravenously with 10 to 20 mCi (370–740 MBq) of technetium-labeled diphosphonate (Table 1-2). Images are obtained 3 to 4 hours after injection.
Indications:
Primary or metastatic bone lesions
Subtle fractures, i.e., stress fractures
Battered child
Bone pain
Three-phase bone scans are performed using the same radiopharmaceutical, but with a different imaging sequence. Blood flow images are obtained in the initial 60 seconds after injection, followed by blood-pool images 2 to 5 minutes after injection and delayed images at 3 to 5 hours.
TABLE 1-2 RADIOPHARMACEUTICALS FOR MUSCULOSKELETAL IMAGING | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
Indications:
Stress fractures
Differentiation of osteomyelitis from cellulitis
Detection of infarction or avascular necrosis
Evaluation of reflex sympathetic dystrophy
Evaluation of peripheral vascular disease
Single-photon emission (computed tomography [CT]) can be used in addition to conventional delayed bone imaging to define subtle lesions, such as pars defects in patients with low-back pain. Computers reconstruct images in multiple planes.
Bone Marrow Imaging
Patients are injected intravenously with 10 to 15 mCi (370–555 MBq) of technetium-labeled sulfur colloid. Images are obtained approximately 15 minutes after injection. Lead shields are placed over the abdomen to delete counts from the liver and spleen.
Indications:
Identify marrow replacement by neoplasms
Define marrow replacement around joint prostheses
Infection
Special approaches may be required for specific indications, such as infection. Several radiopharmaceuticals have been used in this setting. Three-phase bone scans are sensitive, but not specific. White blood cells labeled with gallium-67 citrate and indium-111 or technetium-99m provide more specificity.
Indium-111–labeled leukocyte scans are performed 18 to 24 hours after intravenous injection of 500 mCi (18.5 MBq). Technetium-labeled white cell or antigranulocyte antibody imaging can be performed in 2 to 4 hours. This isotope is more available, and image resolution is superior to that obtained by indium-111 studies. A disadvantage of technetium is biliary excretion into bowel, which may obscure portions of the spine and pelvis.
Gallium-67 citrate scans are performed after 5 to 10 mCi (185–370 MBq) of gallium-67 citrate is injected intravenously. Scanning is performed 24 to 72 hours after injection.
Combined Studies
Use of multiple radiopharmaceuticals may be required for special clinical situations, such as failed joint prosthesis or osteomyelitis. Combined technetium sulfur colloid and indium-111–labeled leukocytes is useful for evaluating loosening or infection of joint prosthesis. Combined technetium-99m diphosphonate and indium-111–labeled leukocytes is useful for osteomyelitis.
Positron Emission Tomography
Positron emission tomography (PET) has provided a new physiologic approach to imaging musculoskeletal disorders, specifically infection and neoplasms.
Positron-emitting agents include fluorine-18-deoxyglucose, L-methyl-carbon 11-methionine, and oxygen 15. Fluorine-18 has a half-life of 110 minutes compared with the shorter half-life of 20 and 21 minutes, respectively, for the other agents. Therefore, fluorine-18 is used clinically. Fluorine-18 fluorodeoxyglucose imaging demonstrates increased glucose use seen with these active processes. Patients must fast for 4 hours before the examination. No sugared beverages should be taken. Normal blood glucose levels are optimal. Scanning is performed 1 hour after injection. Images are evaluated, and uptake ratios of abnormal to normal tissues can be calculated. Early studies demonstrate that PET imaging is more accurate than combined studies described above for evaluating infection, chronic infection, and infection associated with joint replacement arthroplasties. PET is also more useful than conventional radionuclide studies for detection of tumor activity and metastasis.
Positron-emitting agents include fluorine-18-deoxyglucose, L-methyl-carbon 11-methionine, and oxygen 15. Fluorine-18 has a half-life of 110 minutes compared with the shorter half-life of 20 and 21 minutes, respectively, for the other agents. Therefore, fluorine-18 is used clinically. Fluorine-18 fluorodeoxyglucose imaging demonstrates increased glucose use seen with these active processes. Patients must fast for 4 hours before the examination. No sugared beverages should be taken. Normal blood glucose levels are optimal. Scanning is performed 1 hour after injection. Images are evaluated, and uptake ratios of abnormal to normal tissues can be calculated. Early studies demonstrate that PET imaging is more accurate than combined studies described above for evaluating infection, chronic infection, and infection associated with joint replacement arthroplasties. PET is also more useful than conventional radionuclide studies for detection of tumor activity and metastasis.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


