George M. Bridgeforth, David Roberts, and Charles Carroll IV
A 48-year-old man has caught his left middle finger in a machine at work. He complains of marked pain, swelling, and tenderness of his fingertip. He denies any coldness, numbness, or discoloration.

CLINICAL POINTS
- Tuft fractures are comminuted fractures of the distal phalanx.
- The most common cause of these fractures is a crush injury.
- Dislocations are more common at the proximal interphalangeal joint and relatively rare at the distal interphalangeal joint.
Clinical Presentation
Tuft fractures are most commonly comminuted fractures of the distal phalanx. Common sports- and work-related injuries, tuft fractures account for approximately 50% of all hand fractures. The thumb, index, and middle fingers are most frequently involved because they extend the most during usual activities. Crush injuries are the most common cause of tuft fractures—a falling object hitting the finger, catching the finger(s) in a machine or door, or hitting the finger(s) with a hammer. Subungual hematomas, which usually accompany tuft fractures, produce a blue-black, tender bruise, which may elevate the nail. The presence of a hematoma indicates a nail bed laceration, another condition that is commonly associated with tuft fractures.
Pain, swelling, and tenderness are characteristic. Most patients exhibit pain-limited range of motion. It is necessary to evaluate flexor and extensor tendon function by observing ability to actively extend and flex distal interphalangeal (DIP) joint. In addition, it is essential to check neurovascular status carefully:
- Observe skin color, warmth, and capillary refill to assess blood flow.
- Evaluate sensation to light touch and two-point discrimination to assess integrity of the digital nerves.
- Beware of a cold, dusky, cyanotic, numb finger!
A mallet finger, a fingertip injury, is characterized by a flexed posture at the DIP joint and inability to actively extend the finger at the DIP joint. For more information about mallet finger injuries, see Chapter 47.
PATIENT ASSESSMENT 
- Marked pain and tenderness of the distal phalanx
- Swelling, ecchymosis, skin abrasions, and deformity of the distal phalanx
- Limited range of motion
Radiographic Evaluation
For isolated finger injuries, three radiographic views are necessary: posteroanterior (PA), lateral, and oblique (Fig. 46.1A–C). Hand and/or wrist radiographs may be necessary for fractures of multiple digits or other associated injuries.
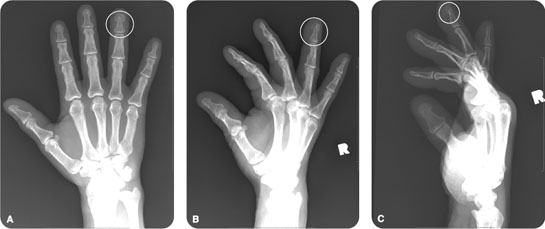
FIGURE 46.1 A 57-year-old man was lifting a heavy object when the object slipped and crushed his right ring finger. (A–C) AP, oblique, and lateral radiographs of the right hand demonstrate an acute fracture of the right fourth phalangeal tuft (circled).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


