Fig. 4.1
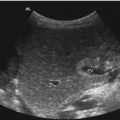
(a) Transverse section of the thyroid gland (panorama view). The thyroid shows homogeneous echotexture. CA common carotid artery, JV jugular vein, SCM sternocleidomastoid muscle, T trachea. (b) Longitudinal section through a normal-sized juvenile thyroid. The image shows homogeneous echogenicity. (c, d) Longitudinal (c) and transverse (d) section through the thyroid gland with measurements
Judging the thyroid gland, the following questions have to be answered:
Is the thyroid gland localised in normal position or is it localised dystopic?
What is the size of the thyroid (Fig. 4.1c, d)? Is the thyroid normal sized or too large or too small?
Anterior and lateral to the thyroid gland lies the sternocleidomastoid muscle (Fig. 4.1a). Lateral and a little bit posterior are the common carotid artery and the jugular vein (Fig. 4.1a).
How are the internal echoes? Are they homogeneous or inhomogeneous? The normal thyroid gland has a homogeneous echotexture without focal hyperechogenic or hypoechogenic areas (Fig. 4.1).
Are there focal lesions? In the positive case, are they cystic or solid? Are solid lesions echogenic or hypoechoic? Do focal solid lesions exhibit calcifications?
Colour Doppler
The arterial supply is provided by the terminal branches of the thyroid artery: The main vascular structure is the superior and inferior thyroid artery, which originate symmetrically from the external carotid artery (Fig. 4.2a). The superior thyroid artery divides into three branches: the superficial, medial and posterior. The inferior artery originates symmetrically from the subclavian artery (Fig. 4.2a). It divides into three branches: medial, inferior and posterior. The main blood supply of the thyroid is represented by the superior thyroid artery.

Fig. 4.2
Doppler sonography of the flow in the thyroid gland. (a) Transverse section through the left globe of the thyroid shows a 2D image of the inferior thyroidal artery (arrows) originating from the common carotid artery. (b) Colour Doppler of the flow in the thyroid gland and the common carotid artery and the jugular vein. The thyroid gland shows only minimal perfusion. As the transducer is tilted cranial, the jugular vein is displayed red and the common carotid artery blue. Due to low-flow settings (6.4 cm/s), aliasing occurs. (c) Pulsed Doppler sonographic flow measurement in a small internal thyroid artery. The flow spectrum is characterised by high diastolic amplitude caused by low peripheral resistance. (d) Doppler sonographic flow measurement in a small thyroidal vein. The complex flow profile is influenced by atrial contractions and respiration
The venous drainage of the thyroid gland begins from a dense subcapsular plexus, which divides into three trunks on each side: the superior thyroid vein, the middle thyroid vein and the inferior thyroid vein.
After 2D imaging, vascularisation of the thyroid has to be judged. As mentioned previously, a low Nyquist limit ≤2 cm/s and a low wall filter ≤100 Hz have to be used. If low-flow settings are used, only few internal vessels can be seen in longitudinal or transverse sections in healthy individuals (Fig. 4.2b). Vascularisation of the thyroid gland is judged as normal, increased or decreased in comparison to the vascularisation of the normal thyroid gland and the neighbouring muscles. In contrast to the few internal vessels of the gland, the flow in the great arteries and veins of the neck is prominently displayed red and blue (Fig. 4.2b).
Spectral Doppler
Internal vessels can be differentiated by pulsed Doppler in arteries and veins. Under normal circumstances, internal thyroid arteries exhibit systolic-diastolic forward flow with high diastolic amplitude, typical to low-resistance arteries (Fig. 4.2c). Veins however have a more complex flow profile with undulations of the amplitude, which are triggered by respiratory movements and atrial contractions (Fig. 4.2d).
4.2 Pathologic Indications
The most frequent indications for sonography and Doppler sonography of the neck are space-occupying lesions of the neck such as enlarged lymph nodes, medial or lateral cervical cysts or fibromatosis colli. These lesions have to be distinguished from the central organ of the neck, the thyroid gland. Doppler sonography is especially helpful for the judgement of the perfusion of lymph nodes and the thyroid gland.
4.2.1 Diseases of the Thyroid Gland
Diseases of the thyroid gland can be differentiated into diffuse or focal pathology.
Diffuse Pathology
Diseases with diffuse pathology are juvenile goitre and autoimmune diseases of the thyroid gland such as Graves’ disease and Hashimoto’s thyroiditis.
In all above-mentioned diseases, the thyroid gland is enlarged. The volume lies over the 97th percentile.
Juvenile goitre is characterised by homogeneous internal echoes and normal vascularisation. Autoimmune thyroiditis is characterised by inhomogeneous echotexture with multiple hypoechoic areas and increased vascularisation (Figs. 4.3, 4.4, and 4.5).



Fig. 4.3
(a, b) Autoimmune thyroiditis. Increased size of the thyroid. The lobulised organ is hypoechoic and shows multiple tiny septa: a, transverse. 1 and 2 the size of the thyroid gland in transverse section; b, longitudinal section. (c–e) Colour Doppler (c, d) and power Doppler (e) show multiple internal vessels indicating increased perfusion of the organ which is characteristic of autoimmune thyroiditis
Fig. 4.4
(a) Hashimoto’s thyroiditis in a 19-year-old boy. Inhomogeneous echogenicity of the large organ with hypoechoic areas within the thyroid and small echogenic septa. (b) Colour Doppler shows increased vascularity characteristic of Hashimoto’s thyroiditis
Fig. 4.5
Graves’ disease in a 17-year-old girl with hyperthyreosis. (a, b) Transverse section of the neck shows a marked increased organ. In contrast to autoimmune thyroiditis, the echogenicity is slightly increased. In contrast to Hashimoto’s thyroiditis, no lobulation can be found. In the centre of the thyroid, an area of focal decreased echogenicity is located. (c) Longitudinal section of the enlarged thyroid with slightly increased echogenicity and inhomogeneous internal echoes. (d) Colour Doppler of Graves’ disease shows marked increased vascularity, the ‘thyroid inferno’. (e) Transverse section through thyroid gland in a 9-year-old girl with Graves’ disease shows an increased organ with homogeneous echotexture and slightly increased echogenicity (Courtesy: Dr. Jüngert, Erlangen). (f) Colour-coded Doppler sonogram of the same patient shows marked increased flow, the ‘thyroid inferno’ (Courtesy: Dr. Jüngert, Erlangen)
4.2.1.1 Hashimoto’s Thyroiditis
Chronic lymphocytic thyroiditis is an autoimmune disease that affects especially female adolescents. One-third of the patients have associated functional disorders such as hypothyroidism or hyperthyroidism (Bruneton et al. 2002a, b).
2D Image
The thyroid of patients with Hashimoto’s thyroiditis is enlarged. The echogenicity varies from hypoechoic to hyperechoic depending on the stage of the disease. High-resolution transducers of 10 MHz and more can depict multiple micronodules of 1–6 mm in diameter (Fig. 4.3a, b) (Set et al. 1996). The micronodules are surrounded by echogenic halos due to increased lobulation (Sostre and Reyes 1991). Micronodules have a predictive value of Hashimoto’s disease of 94.7 % (Yeh et al. 1996).
Messina (1999) classified sonographic patterns of Hashimoto’s thyroiditis in four groups:
Colour Doppler Sonography
Colour and power Doppler sonography is helpful for the differentiation of Hashimoto’s thyroiditis from Graves’ disease. In Hashimoto’s thyroiditis, the flow is normal in 49 % of cases and slightly increased in 44 % (Fig. 4.3c–e) (Bruneton et al. 2002a, b). This clearly distinguishes Hashimoto’s disease from Graves’ disease which always shows increased vascularity (Fig. 4.5d). In our experience, both diseases are characterised by increased vascularity. Therefore, colour Doppler is not a good method to differentiate both entities. In comparison with Graves’ disease, hypervascularity in Hashimoto’s thyroiditis is not so pronounced as in Graves’ disease.
4.2.1.2 Graves’ Disease (Basedow’s Goitre)
Besides Hashimoto’s thyroiditis, Graves’ disease is the second most frequent form of autoimmune disorder. Coexistence with other autoimmune disorders exists.
2D Image
Colour and Pulsed Doppler
Colour Doppler shows increased vascularity, the so-called thyroid inferno (Fig. 4.5d) (Ralls et al. 1988).
The increased vascularity is due to numerous arteriovenous shunts. Hypervascularisation is caused by the autoimmune process.
Differentiation Between Hashimoto’s Thyroiditis and Graves’ Disease
Neither 2D images nor colour Doppler can distinguish between both forms of autoimmune thyroiditis for sure. Only clinical and laboratory investigations can differentiate both diseases:
Graves’ disease is characterised by increased TSH receptor antibodies, an increase of T3 and T4 and a decrease of TSH.
Hashimoto’s thyroiditis is characterised by an increase of microsomal and thyroglobulin antibodies and normal or decreased T3 and T4 levels and normal or increased TSH levels.
Focal Pathology
One-third of normal people over 40 years have one or more nodular lesions of the thyroid. The number increases with age. Focal lesions can be benign or malignant. Fortunately, malignant lesions rarely occur in childhood (0.004 % per year) (Gharib 1994). Dependent on the echogenicity, delineation and vascularity, benign and malignant lesions can be differentiated.
2D Image and Doppler Sonography
Focal lesions within the thyroid increase with age. They arise especially in patients who suffer from iodine deficiency.
Focal lesions of the thyroid gland can be echo-free and echogenic or have normal echogenicity.
Echo-free lesions are almost always benign.
Echogenic lesions may be benign or malignant.
Most thyroid nodules are hypoechoic. Rarely are they hyperechoic or have similar echogenicity as the thyroid.
Solid lesions in the thyroid occur with a frequency of 0.2–1.5 % in the paediatric population (Hung et al. 1992; Raab et al. 1995).
Most solid tumours of the thyroid are benign although an incidence of 2–40 % of malignancy has been reported (Hung et al. 1992; Raab et al. 1995).
Malignancy occurs especially in children and elder people. Focal lesions which occur in males are more probably malignant than in females.
Table 4.1 summarises benign and malignant focal lesions.
Table 4.1
Focal lesions of the thyroid
Benign | Malignant |
|---|---|
Focal goitre | Papillary carcinoma |
Simple cyst | Follicular carcinoma |
Haemorrhagic cyst | Medullary carcinoma |
Adenoma | Undifferentiated carcinoma |
Non-Hodgkin’s lymphoma | |
Metastases | |
Haemangioendothelioma |
4.2.1.3 Cysts
Echo-free lesions are simple cysts. They do not show internal echoes (Fig. 4.6). True epithelium-lined simple cysts represent only 1 % of all benign thyroid masses (Siegel 2002a, b). Most cysts are probably the result of cystic degeneration of follicular adenomas, rather than true cysts (Siegel 2002a, b). Large cysts may develop internal haemorrhage (Fig. 4.7a). Haemorrhagic cysts exhibit sedimentation of internal echoes. Most haemorrhagic cysts correspond to solid lesions that have undergone necrosis and cystic degeneration (Fig. 4.7). Without motion, the internal echoes form a linear surface. The sedimentation is caused by erythrocytes or crystals. During motion, the echoes fill the cyst like a snow storm. The haemorrhagic lesion may form a complex mass with echo-free, hypoechoic and echogenic areas (Fig. 4.7a).


Fig. 4.6
(a) Transverse section of a large thyroid cyst. The band-like internal structures near the wall of the cyst represent fibrin strands. Additionally, focal increased echogenicity can be found. (b) Colour Doppler shows no vessels within the cyst
Fig. 4.7
(a) Haemorrhage in a large cyst in a 14-year-old boy. The transverse section shows a complex mass with multiple floating internal echoes (erythrocytes) and fibrin strands. (b, c) Colour Doppler shows no internal vessels. Only the border zones of the cyst are vascularised: b, longitudinal; c transverse section
Echogenic lesions may be benign or malignant. The echotexture may be homogeneous or inhomogeneous. Complex nodular masses of the thyroid occur in about 25 % of all thyroid nodules (Bruneton et al. 2002a, b).
4.2.1.4 Adenomas
Adenomas are the most common cause of a solid thyroid nodule in childhood (Hung et al. 1992).
2D Sonography
Adenomas are solitary, well-encapsulated lesions in an otherwise normal thyroid gland. Most adenomas are hypoechoic in comparison to the remaining thyroid. Some are hyperechoic and a few isoechoic (Siegel 2002a, b). Adenomas may have heterogeneous echogenicity with echogenic solid and echo-free cystic areas (Figs. 4.8, 4.9, 4.10 and 4.11). Internal calcifications are usually absent; if present they are suspicious of a malignant lesion (Fig. 4.12). Missing calcifications are a very sensitive sign of benignity.





Fig. 4.8
(a) Adenoma of the thyroid in a 14-year-old female. The transverse section of the thyroid shows a focal lesion with normal internal echoes. A complete hypoechoic rim can be shown which is typical of an adenoma. The hypoechoic halo is formed by a ring of vessels which can excellently be shown by colour Doppler. (b) Colour Doppler. The hypoechoic halo is formed by a vascular ring, which is typical for adenomas
Fig. 4.9
(a, b) Adenoma of the thyroid in a 32-year-old female. The longitudinal (a) and transverse (b) sections show a focal lesion with inhomogeneous internal echoes. The lesion is surrounded by a complete hypoechoic ring and contains several small cystic areas. (c) Colour Doppler shows marked perfusion of the tumour with a vascular ring characteristic of an adenoma. (d) Pulsed Doppler recording of the flow in the vascular ring shows antegrade systolic-diastolic flow with a high diastolic amplitude, characteristic of low peripheral vascular resistance
Fig. 4.10
Macrofollicular adenoma in an 11-year-old girl. (a) Transverse image of a partially cystic tumour in the left lobe of the thyroid. The node is surrounded by a hypoechoic rim and consists to 3/4 of solid elements. (b, c) Colour Doppler shows increased perfusion of the tumour
Fig. 4.11
Thyroid adenoma in 25-year-old young man. (a) Longitudinal scan through the right thyroid shows a hypoechoic mass with multiple microcystic areas and dorsal acoustic enhancement. (b, c) Colour Doppler (b) and power Doppler (c) show increased vascularity of the tumour characteristic of an adenomatous nodule. (d) Spectral Doppler of the arterial flow in the solid elements shows increased diastolic flow due to low peripheral resistance
Fig. 4.12
(a) 2D image of a papillary carcinoma of the thyroid (longitudinal section). The image shows an incomplete halo and inhomogeneous internal echoes. If the halo is incomplete, it is suspicious of a malignant tumour. (b, c) 2D image of a papillary carcinoma of the thyroid in a 5-year-old girl. The tumour has invaded the complete left lobe (markers). It is characterised by heterogeneous reflexes and multiple spot-like calcifications which are suspicious of malignancy (arrows). (d) Colour Doppler of the perfusion of the organ. The tumour is richly vascularised. It shows multiple pathologic vessels invading the tumour from the capsule. (e) Medullary carcinoma of the thyroid (transverse section). The left lobe is enlarged due to invasion by a hypoechoic tumour which is characterised by inhomogeneous internal echoes. Suspicious of malignancy are the small focal areas of calcification (arrows) (Courtesy Dr. Hammersen, Nürnberg)
Sixty percent of the adenomas have a thin hypoechoic rim (halo) around the lesion (Fig. 4.8a).
A complete hypoechoic halo which surrounds a homogeneous lesion is a sign of benignity (Figs. 4.8a, 4.9a, b and 4.10a) (Seya et al. 1990). On the other hand is an incomplete halo or a missing halo, a strong hint for malignancy (Figs. 4.12a and 4.13a) (Rago et al. 1998). A complete rim around the tumour is characteristic of a follicular adenoma (Figs. 4.8a, 4.9a, b and 4.10a). It is found in about 60 % of follicular adenomas (Siegel 2002a, b). The cause of the rim is not clear. It may be caused by the fibrous capsule, compressed thyroid parenchyma, pericapsular inflammatory infiltrate or vessels which surround the nodule (Fig. 4.8b) (Siegel 2002a, b).

Fig. 4.13
(a) Folliculary carcinoma of the thyroid in a 15-year-old girl with autoimmune thyroiditis, who developed two focal lesions in the thyroid. The tumours have mixed echogenicity with focal echogenic and focal hypoechoic areas. (b) Colour Doppler reveals pathologic vessels and marked increased vascularity (type 3) (Courtesy Dr. Ludwig von Rohden, Magdeburg)
Doppler Sonography
Colour Doppler and power Doppler sonography reveals if the halo is formed by a vascular ring (Fig. 4.8b). Adenomas show increased vascularity in comparison with the normal thyroid (Figs. 4.9c, 4.10b, c and 4.11b, c).
Pulsed Doppler shows systolic-diastolic forward flow with high diastolic amplitude due to low peripheral resistance (Fig. 4.11d).
Haemorrhage into an Adenoma
If bleeding occurs into follicular adenomas, the focal lesion may appear as a complex tumour (Fig. 4.7). Haemorrhage may be caused by simple trauma or occur spontaneously. During time, the lesion gets more and more hypoechoic. Complex tumours with inhomogeneous echotexture (25 %) and a fluid component of two-thirds are almost always necrotic, benign lesions (Fig. 4.7) (Viateau-Poncin 1992).
Thyroid Malignancy
2D Sonography
Most thyroid cancers appear as hypoechoic nodules in comparison with the normal thyroid parenchyma. Less commonly they are hyperechoic or isoechoic (Siegel 2002a, b). The margins of the tumour vary from irregular and ill defined to smooth and well delineated (Figs. 4.12 and 4.13) (Siegel 2002a, b). If a sonolucent rim or halo can be found, it is usually incomplete and only partially surrounds the lesion (Figs. 4.12a and 4.13a). By high-resolution linear transducers of 10 MHz, more microscopic calcifications can be detected as punctuate echogenic foci without acoustic shadowing (Fig. 4.12c, e). They are characteristic of thyroid cancer but cannot distinguish between the different forms of malignancy.
If the tumour has inhomogeneous internal echoes, is hypoechoic and exhibits focal calcifications, malignancy is most probable (Figs. 4.12 and 4.13) (Lee et al. 1993). It is very important however to state that microcalcifications can only be seen with high-resolution linear transducers of 10 MHz or more (Fig. 4.12) (Bruneton et al. 2002a, b).
Carcinomas of the thyroid rarely occur in infancy and childhood (1:100,000). Only 1–1.5 % of all childhood malignancies which are diagnosed before the age of 15 years are carcinomas of the thyroid (Siegel 2002a, b). Two-thirds of them are found in girls between an age of 7 and 12 years (Siegel 2002a, b).
Papillary thyroid carcinoma is the most common subtype of thyroid cancer in childhood, accounting for 70–90 % of all cases (Moir and Telander 1994).
The most common ultrasound finding is a hypoechoic nodule (86.7 %) (Lu et al. 1994). Nodules over 1 cm are always inhomogeneous with poorly defined margins in 80 % of patients (Fig. 4.12) (Pacella et al. 1998). Less than half of them contain microcalcifications (Fig. 4.12c, e) (Bruneton et al. 2002a, b). Less frequently, cystic degeneration (28.3 %) and the halo sign (13.2 %) can be found (Figs. 4.12a and 4.13a) (Bruneton et al. 2002a, b). Isoechoic or hyperechoic lesions are much rarer (2 %) (Lu et al. 1994). Solid sonographic patterns predominate (85.5 %), whereas mixed patterns (11.7 %) and cystic patterns (2.8 %) are less common (Lin and Huang 1998). Cervical lymph node metastases occur in 63.8 % of papillary carcinomas (Sugino et al. 1998). They are usually hyperechoic and homogeneous (81.2 %) (Ahuja et al. 1995).
Follicular carcinoma accounts for 10–20 % of all thyroid malignancies (Siegel 2002a, b). This rare carcinoma is isoechoic or less often hypoechoic (Fig. 4.13). Neither microcalcification nor cervical lymphadenopathy is present (Bruneton et al. 2002a, b). In the series of Lin et al. (1997), 76.2 % of all follicular cancers presented as a hypoechoic nodule.
Medullar carcinoma comprises between 1 and 10 % of thyroid cancers in children (Siegel 2002a, b). Sonographically, medullary carcinomas are hypoechoic. Microcalcifications exist in 80–90 % of all cases (Fig. 4.12e) (Gorman et al. 1987). Laterocervical lymphadenopathy frequently occurs.
Differential diagnosis between the different forms of thyroid malignancy is not possible with sonography alone. In some cases, colour and power Doppler is helpful for further differential diagnosis.
Doppler Sonography
Solbiati et al. (1995) described attempts to differentiate benign and malignant lesions according to colour and power Doppler.
Echo-free lesions do not show vascularity if colour or power Doppler is used. An echo-free focal lesion without vascularity nearly always is benign.
Echogenic lesions may have an increased, normal or a decreased vascularity in comparison with the normal thyroid gland.
Solbiati described three types of vascularity:
Type 1: Avascular lesions
Type 2: Peripheral vascularisation
Type 3: Mixed (peripheral and central) vascularisation
Ad 1: Cysts are avascular (type 1).
Avascular nodules are the only consistent benign lesions and correspond to follicular hyperplasia (Argalia et al. 1995).
Ad 2: Peripheral vascularisation (type 2) is typical for adenomas (Figs. 4.8b and 4.9c). The characteristic echo-poor rim may be caused by vessels which surround the adenoma (Figs. 4.8b and 4.9c). CD demonstration of a complete halo which contains vascular structures around a nodule is highly specific of benignity (sensitivity 96 %, specificity 93 %) (Stern et al. 1994).
Ad 3: Solid lesions with extensive internal vascularisation and peripheral and central vessels almost always are malignant (Figs. 4.12d and 4.13b). Type 3 vascularisation could never be seen in benign lesions (Siegel 2002a, b). High-grade internal vascularisation has a positive predictive value in the diagnosis of thyroid malignancy (Messina et al. 1998). The combination of an absent halo sign, microcalcifications on ultrasound and marked intranodal blood flow has a high specificity for malignancy (97.2 %) but only a sensitivity of 16.6 % (Siegel 2002a, b).
No correlation between morphology, function and scintigraphy exists. Additionally no correlation between colour Doppler (hypervascularity), scintigraphy and laboratory values exists (Bruneton et al. 2002a, b).
In summary, the following differential criteria between benignity and malignancy exist (Table 4.2) (Bruneton et al. 2002a, b):
Table 4.2
Sonographic and Doppler sonographic characteristics of benign focal lesions in the thyroid
Hyperechoic or at least 2/3 cystic lesion |
Complete halo |
No calcifications |
Not hypervascular |
Not associated with cervical lymphadenopathy |
A lesion is most likely benign if:
It is hyperechoic or cystic (at least 2/3).
It has a complete halo.
It has no calcifications.
It is not hypervascular.
It is not associated with cervical lymphadenopathy.
A lesion should be considered malignant (Table 4.3) if:
Table 4.3
Sonographic and Doppler sonographic characteristics of malignant focal lesions in the thyroid
Hypoechoic with inhomogeneous echogenicity |
No complete halo |
Microcalcifications |
Irregular central hypervascularity |
Association with cervical lymphadenopathy |
Poorly defined margins |
It is hypoechoic with inhomogeneous echogenicity and irregular margins.
It has no complete halo.
It exhibits microcalcifications.
It shows irregular central hypervascularity.
It is associated with cervical lymphadenopathy.
Predictive value for malignancy is only high if multiple sonographic signs at greyscale and colour Doppler are present in a thyroid nodule. Unfortunately, not all focal lesions of the thyroid exhibit characteristic signs of benignity or malignancy.
In all unclear cases of focal lesions of the thyroid, fine needle biopsy or surgical resection of the nodule should be performed.
4.2.2 Cervical Lymphadenopathy
Apart from thyroid sonography, cervical lymphadenopathy is the most frequent indication of cervical sonography.
Palpation is the first method for investigation of the neck. But even if the palpation is performed by an experienced examiner, the exact number and extension of an existing lymphadenopathy can never be estimated.
The head and neck region contains the largest number of lymph nodes (approximately 400–700) (Bruneton et al. 2002a, b).
Six levels of lymphadenopathy can be differentiated:
Level 1: Submental and submandibular nodes
Level 2: High jugular nodes
Level 3: Mid-jugular nodes
Level 4: Low jugular nodes
Level 5: Spinal accessory and transverse cervical nodes
Level 6: Anterior cervical nodes
From the clinical point of view, the neck can be divided into the posterior and anterior triangles anatomically. The division is made by the sternocleidomastoid muscle. The lymph nodes located in the posterior triangle tend to be benign (Dehner 1987).
Infectious lymphadenopathy is very frequent in paediatrics. Diagnosis is usually made clinically. Ultrasound is not of diagnostic value itself, but can be useful in large lymph nodes to search for abscess formation and for the delineation from surrounding tissues.
Enlarged cervical lymph nodes, due to common infections, usually occur below the angle of the mandible and in the jugulo-carotid region (Geoffray and Garel 2002).
An important question in the paediatric patient is if an enlarged lymph node is benign or malignant.
Apart from 2D imaging, colour Doppler and PW Doppler are very helpful to differentiate benignity and malignancy.
2D Image
The investigation has to be performed with high-resolution linear transducers with a frequency of at least 10 MHz. Higher-frequency transducers (>10 MHz) allow better detail resolution. The superficial cervical lymph nodes are best examined after visualisation of the common carotid artery (CCA) and the internal jugular vein (IJV). Axial scans, obtained along the transverse axis of the vessels, permit satisfactory evaluation of the vascular relationship of any nodal mass. Sonography depicts the nodes of levels 2, 3 and 4 which lie anterior to the CCA and IJV.
The lymph nodes of level 5 lie behind these two vascular structures.
Normal cervical lymph nodes are oval and hypoechoic with an echogenic linear hilus which contains the vascular pedicle (Figs. 4.16, 4.18 and 4.19) (Bruneton et al. 1994; Ying et al. 1996). Colour Doppler and power Doppler can identify the central vessels in the hilus of the normal lymph node (Fig. 4.16b).
The differentiation of infectious lymph adenopathies and malignant lymph node affections is important.
A number of parameters permit the differentiation between benign and malignant lesions:
Maximal transverse diameter
Longitudinal/maximal transverse diameter ratio
Nodal hilus
Nodal cortex
Nodal margins
Nodal echotexture
The maximal transverse diameter of more than 0.8 cm in adults is considered the upper limit of a reactive lymphadenopathy (Bruneton et al. 1994). If the lymph node has a diameter over 2 cm, it is obligatory pathologic (in adults). These values however cannot be used in infancy and childhood.
Longitudinal/maximal transverse diameter ratio is the most sensitive greyscale imaging method to differentiate malignancy and benignity. Benign lymph nodes tend to be oval, whereas malignant nodes are more round. Malignant lymph nodes have a mean L/T ratio of 1.4, whereas benign nodes have mean ratio of 1.9 (Chang et al. 1994).
The calculation of the short/long axis ratio of Ying et al. (1999) defined the optimal cut-off value for the different cervical regions: submental nodes 0.5; submandibular nodes 0.7; parotid nodes 0.5; upper cervical nodes 0.4; middle cervical nodes 0.3; and posterior triangle nodes 0.4.
Hilus: Cervical lymph nodes often have a hyperechoic central line (Fig. 4.20a) that is formed by lymphatic sinuses that converge in the internal portion of the medulla, where it is supported by loose connective tissue (Bruneton et al. 2002a, b). The differential diagnosis of malignancy and benignity is not always possible, although the hyperechoic line often is indicative of reactive aetiology.
The thickness of the nodal cortex can only be assessed if the hilus is echogenic. A narrow cortex (thickness half the transverse diameter of the hilus) is typical for benign nodes. Concentric cortical widening can essentially be found in malignancy. Eccentric cortical widening may be due to focal malignant invasion (Bruneton et al. 2002a, b).
Nodal margins are a poor criterion for discrimination of benignity and malignancy. Surface irregularities and blurred margins nearly always correspond to capsular rupture of metastases, regardless of size (Fig. 4.26a, b) (Bruneton et al. 2002a, b).
The internal nodal echotexture of normal and reactive lymph nodes is constant. It exists on a hypoechoic cortex and a hyperechogenic hilus similar to a tree with a trunk and treetop (Fig. 4.20a). The cortex is hypoechoic in comparison to fat and surrounding connective tissue.
Marked hypoechogenicity may be found in lymphoma (Figs. 4.24a, 4.25a, and 4.26a). In contrast to adults, where metastatic lymph nodes may occur, this is very rare in infants and children. Most forms of lymphadenitis in infancy and childhood are reactive. They are caused by either bacterial or viral infections. In bacterial lymphadenitis, abscess formation may develop. It is characterised by a liquid centrum surrounded by hypoechoic tissue (Fig. 4.17). Gas-producing bacteria may cause focal areas of increased echogenicity scattered in the enlarged lymph nodes. Colour Doppler is very helpful for the differential diagnosis of abscesses and reactive lymphadenitis (Figs. 4.15, 4.16, and 4.17). In areas of abscess formation, colour Doppler or power Doppler shows no vessels (Fig. 4.17b, c).
The best 2D criterion to differentiate benignity and malignancy is the hyperechoic central line and the transverse diameter (Figs. 4.20a and 4.24a). Absent hilus echoes and increase in the short axis length are suspicious of malignancy (Figs. 4.23, 4.24, and 4.25) (Chicui et al. 2000).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


