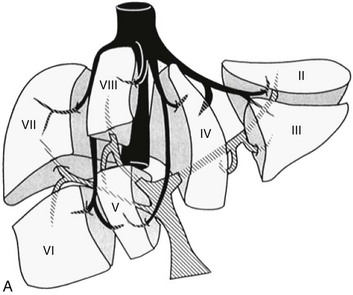
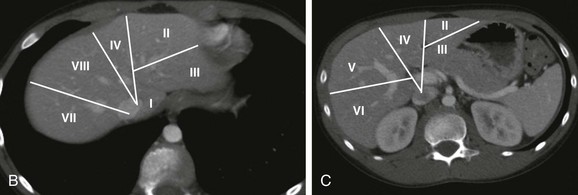
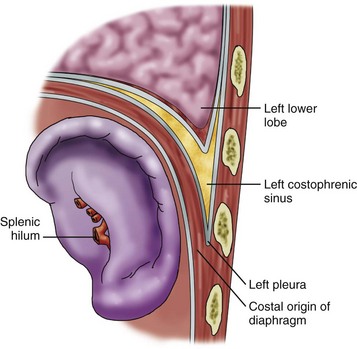
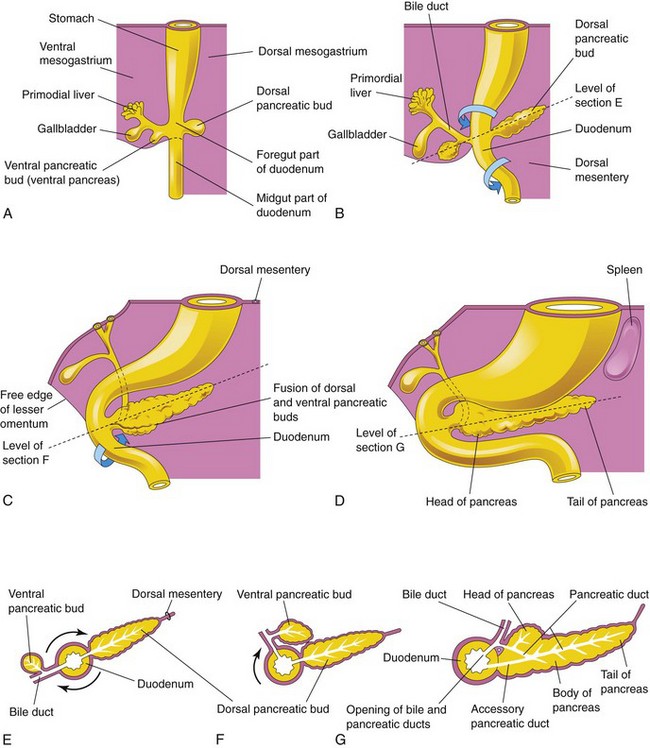
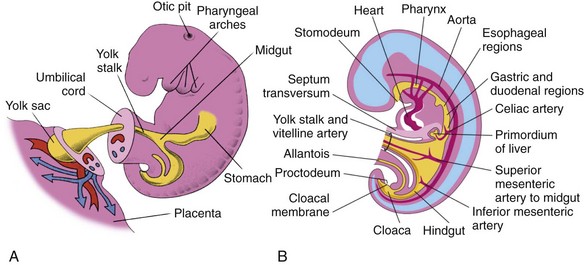
Chapter 84 During the third week of gestation the intraembryonic mesoderm differentiates, forming the lateral plates.1,2 Mesoderm from paravertebral myotomes invades the lateral plates during the sixth week. The leading edges of the lateral plates will differentiate into the right and left rectus abdominis muscles. The main portion of the mesoderm splits into three layers and forms the external oblique, internal oblique, and transverse abdominis muscles. Approximation of the right and left recti is complete by the twelfth week except for the umbilical ring. The aponeurosis of the external oblique muscles forms the anterior and posterior rectus sheaths.1 These sheaths join in the midline to form the linea alba. The lowest portion of the aponeurosis ends in the inguinal ligament. The external inguinal ring is an opening in the aponeurosis between the inguinal ligament inferiorly and the tendinous portion superiorly. The spermatic cord in males and the round ligament in females pass through the inguinal canal. Closure of the cephalic, caudal, and lateral folds leads to the formation of the intraembryonic coelom.3,4 The mesoderm surrounding the coelom splits into two layers, the somatic mesoderm and the splanchnic mesoderm. The somatic layer forms the parietal peritoneum, which lines the inner abdominal wall, and the splanchnic layer forms the visceral peritoneum, which covers the abdominal organs. The space between the parietal and visceral peritoneum is the peritoneal cavity. The liver, gallbladder, and biliary duct system arise as a ventral outgrowth from the caudal end of the foregut early in the fourth week of development (Fig. 84-1).5,6 This outgrowth, known as the hepatic diverticulum, extends into the septum transversum, which is the future diaphragm. The hepatic diverticulum grows rapidly and divides into cranial and caudal portions. The larger cranial portion forms the primordium of the liver parenchyma. Proliferating endodermal cells develop into cords of hepatocytes and into the epithelial lining of the biliary system. The connective tissue, hematopoietic cells, and Kupffer cells are derived from the mesoderm of the septum transversum. The caudal portion expands to form the gallbladder, and its stalk becomes the cystic duct. The two major intrahepatic ducts join to form the common hepatic duct. The stalk connecting the hepatic and cystic ducts to the duodenum becomes the common bile duct. Figure 84-1 Schematic illustrations of hepatic embryology. The liver is the largest of the abdominal organs, with the right lobe being larger than the left lobe.7 It occupies most of the right upper quadrant, extends across the midline, and is relatively larger in infants than in older children and adults. The superior portion of the liver is in direct contact with the diaphragm and is known as the bare area because it is not covered by peritoneum. The posterior margin abuts the inferior vena cava, the right adrenal gland, and the distal esophagus. Inferiorly, the liver is in contact with the colon, gallbladder, and right kidney. The left lobe is in contact with the stomach. The visceral surface of the liver contains the porta hepatis with its vessels and biliary ducts. Traditional nomenclature in the United States divides the liver into five segments. However, hepatic segmental anatomy as described by Couinaud is more useful in defining surgically resectable segments (Fig. 84-2).8 In Couinaud’s system, the right and left lobes of the liver are divided by the middle hepatic vein and the Cantlie line, a line between the inferior vena cava and the gallbladder fossa. The caudate lobe is segment I. Segments II to IV are in the left lobe and segments V to VIII are in the right lobe. The left hepatic vein divides the left lobe into posterior segment II and anterior segments III and IV; segments III and IV are separated by the umbilical fissure and falciform ligament. The right hepatic vein divides the right lobe into posterior segments VI and VII and anterior segments V and VIII. The superior segments (VII and VIII) are separated from the inferior segments (V and VI) by the right portal vein. The spleen begins to develop during the fifth week of gestation.9,10 It is derived from a mass of mesenchymal cells in the dorsal mesogastrium that coalesce to form the spleen. Failure of these cells to fuse completely gives rise to accessory spleens, which are quite common. As the stomach’s greater curvature rotates to the left, the spleen is carried with it into the left upper quadrant. It lies in a niche formed by the diaphragm, the stomach, the left kidney and adrenal gland, the phrenicocolic ligament, and the chest wall (Fig. 84-3). The splenic hilum is a depression along the medial surface through which the splenic artery, vein, and nerves pass. The two major ligaments that hold the spleen in place are the gastrosplenic and the splenorenal ligaments. Other ligaments that support the spleen are the splenophrenic, splenocolic, splenopancreatic, colophrenic, and pancreaticocolic ligaments. The embryonic spleen is a site of hematopoiesis in some mammalian species, such as rodents, but current evidence suggests that splenic hematopoiesis does not occur in the human fetus.11 The spleen is an important lymphatic organ and plays a role in providing protection from infection caused by encapsulated organisms. Lymphocytes begin to appear in the spleen around 11 weeks of gestation. The spleen also filters damaged red blood cells and foreign particles and acts as a reservoir for platelets. The development of the pancreas is closely related to duodenal development. The dorsal pancreatic bud arises from the dorsal side of the duodenum, and the ventral pancreatic bud arises from the liver diverticulum (Fig. 84-4).12–14 The larger dorsal bud appears first and arises cranial to the smaller ventral bud. It will form the tail, body, and part of the head of the pancreas. The ventral bud develops at the site of entry of the common bile duct and forms part of the pancreatic head and the uncinate process. As the duodenal loop rotates, the ventral bud is carried dorsally to lie in a position posterior to the dorsal bud, with which it fuses. After fusion of the pancreatic buds, the duct systems anastomose. The main pancreatic duct is formed proximally from the ventral bud and the distal portion is formed from the dorsal pancreatic bud. The proximal portion of the duct from the dorsal bud either disappears or persists as the accessory pancreatic duct. Islet cells appear at the end of the second month of gestation, and acinar cells develop during the third month. The islet cells secrete insulin, glucagon, somatostatin, and pancreatic polypeptide. Acinar cells produce digestive enzymes that are secreted into the second portion of the duodenum. The pancreas lies horizontally in the retroperitoneum.15 The head of the pancreas lies to the right of the midline in the curve of the duodenum. The uncinate process is an extension of gland substance at the junction of the inferior and left margins of the pancreatic head. The anterior surface of the pancreatic head is in contact with the transverse colon, gastroduodenal artery, and several loops of small intestine. The posterior surface is adjacent to the inferior vena cava, common bile duct, renal veins, and abdominal aorta. The anterior surface of the uncinate process is in contact with the superior mesenteric artery and vein. The primitive gastrointestinal tract forms during the third to fourth week of gestation.16–19 It is marked by the oropharyngeal membrane at the cranial end and the cloacal membrane caudally (Fig. 84-5). It is divided into three parts: the foregut, midgut, and hindgut. The foregut includes the esophagus, stomach, and proximal duodenum and receives most of its arterial supply from the celiac axis, with the exception of the esophagus, which is proximal to the lower esophageal sphincter. The midgut is supplied by the superior mesenteric artery and includes the distal duodenum, jejunum, ileum, cecum, appendix, ascending colon, and approximately two thirds of the transverse colon. The hindgut is supplied by the inferior mesenteric artery and comprises the remainder of the transverse colon, the descending and sigmoid colon, and the upper two thirds of the rectum.
Embryology, Anatomy, and Normal Findings
Abdominal Wall and Peritoneal Cavity
Hepatic and Biliary System
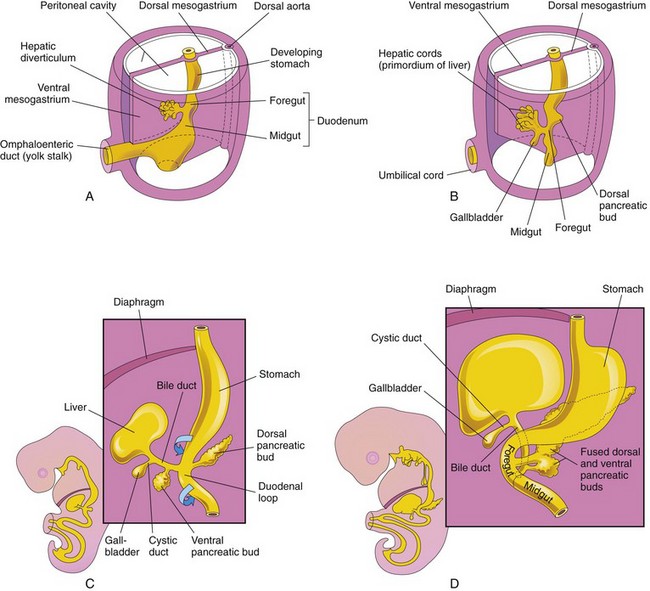
A, Hepatic embryology at 4 weeks. B and C, Hepatic embryology at 5 weeks. D, Hepatic embryology at 6 weeks. Note hepatic diverticulum extending into the ventral mesentery and dividing into cranial (liver primordium) and caudal (gallbladder and common bile duct) buds. Also note that the entrance of the bile duct into the duodenum shifts gradually to a posterior position, which explains why the bile duct passes posterior to the duodenum. (From Moore KL, Persaud TVN. The digestive system. In: Moore KL, Persaud TVN, eds. The developing human: clinically oriented embryology. 8th ed. Philadelphia: WB Saunders; 2007.)
Spleen
Pancreas
Gastrointestinal Tract
Embryology, Anatomy, and Normal Findings