Enhancing (hyperemic) peripheral inner rim (increased vascularity)
Nonenhancing peripheral outer rim or “halo” (avascular rim)
Delayed or nonenhancing central part of tumor (myxoid and hyalinized stroma)
• Imaging protocol: Multiphasic CT or MR
• Spectrum of growth in lesions may be seen: Nodular form (more common); diffuse or extensive form (very rare)
TOP DIFFERENTIAL DIAGNOSES
• Peripheral cholangiocarcinoma
• Treated malignancy
• Focal confluent fibrosis
• Hemangioma (especially in cirrhotic liver)
PATHOLOGY
• Slowly progressing, low-grade, malignant vascular tumor of liver
Most patients survive 5-10 years after diagnosis
• Must not be confused with infantile hemangioendothelioma
Benign primary vascular liver tumor
Resolves spontaneously in many cases
DIAGNOSTIC CHECKLIST
• Usually located at periphery with extension to capsule
• Typical capsular retraction of peripheral tumor (due to fibrosis and ischemia)
Rule out other hepatic lesions that typically cause capsular retraction
• “Target” appearance on CECT or MR
• Differentiated from other lesions by tumor cells staining positive for factor VIII-related antigen
(Left) Axial CECT shows multiple peripheral, hypovascular lesions with a “target” appearance (central lucency), typical CT findings of epithelioid hemangioendothelioma (EHE). The subcapsular lesions are associated with retraction of the overlying liver capsule .
(Right) CT of the same patient shows more of the multicentric “target” lesions typical of EHE, mostly in a peripheral location within the liver.
(Left) Gross pathology of the same liver after explantation shows the “target” appearance of the lesions, with necrosis and white fibrous tissue in the center of the lesions, as well as a peripheral rim of compressed parenchyma and hyperemic tumor.
(Right) Central portion of EHE typically is hypocellular with loosely arranged spindle cells in a fibromyxoid or sclerotic stroma. The findings can simulate a scar or sclerosed hemangioma. (Courtesy S. Kakar, MD.)
TERMINOLOGY
Abbreviations
• Epithelioid hemangioendothelioma (EHE)
Synonyms
• Hepatic epithelioid hemangioendothelioma
Definitions
• Primary malignant tumor of liver arising from vascular elements of mesenchymal tissue
IMAGING
General Features
• Best diagnostic clue
Coalescent peripheral hepatic nodules with target-like appearance and capsular retraction
• Location
Liver
– Periphery (> 75%) with extension to capsule
Locations other than liver
– Soft tissues, bone, and lung
• Size
Varies from small tumor nodules to large confluent masses
• Key concepts
Rare primary malignant (low-grade) vascular tumor of liver in adults
Other primary malignant vascular tumors of liver
– Angiosarcoma (2% of all primary malignant liver tumors)
– Kaposi sarcoma: Metastatic vascular tumor in AIDS and transplant recipients
All hepatic malignant vascular tumors
– Share histologic characteristics
– Grow around and into vessels
– Tend to be multifocal
Clinical course
– Less aggressive than angiosarcomas or hepatocellular carcinoma, but still fatal in most cases
– Variable and unpredictable
– Metastatic in 40% of cases (spleen, mesentery, lymph nodes, lung, bone)
CT Findings
• Spectrum of growth in lesions may be seen
Nodular form (more common)
– Multiple liver nodules coalesce to form large, confluent masses
Diffuse or extensive form (very rare)
• Usually located at periphery with extension to capsule
• Capsular retraction (due to tumor fibrosis and ischemia) or flattening; segmental volume loss
• Occasional calcification within tumor
• Compensatory hypertrophy
Uninvolved liver (usually left lobe)
• May have extrahepatic metastases and ascites
• NECT
Tumor nodules
– Foci of homogeneous decreased attenuation (due to myxoid stroma) compared to normal liver parenchyma
Conspicuity and extent of lesions
– CECT superior to NECT
• CECT
Target-like enhancement pattern of tumor
– Delayed or nonenhancing central part of tumor (myxoid and hyalinized stroma)
– Enhancing (hyperemic) peripheral inner rim (increased vascularity)
– Nonenhancing peripheral outer rim or “halo” (avascular rim)
MR Findings
• T1WI
Lesions are hypointense centrally
Peripheral, thin, hypointense rim
• T2WI
Hyperintense centrally
Peripheral, thin, hypointense rim
• T1WI C+
“Target” pattern: 3 concentric layers of alternating signal intensity (analogous to CECT appearance)
– Center: Hypointense
– Periphery: Thick, enhancing, inner rim and thin, nonenhancing, outer rim
Ultrasonographic Findings
• Grayscale ultrasound
Tumor nodules show varied echogenicity pattern
– Predominantly hypoechoic
Only gold members can continue reading. Log In or Register to continue









 with a “target” appearance (central lucency), typical CT findings of epithelioid hemangioendothelioma (EHE). The subcapsular lesions are associated with retraction of the overlying liver capsule
with a “target” appearance (central lucency), typical CT findings of epithelioid hemangioendothelioma (EHE). The subcapsular lesions are associated with retraction of the overlying liver capsule  .
.
 typical of EHE, mostly in a peripheral location within the liver.
typical of EHE, mostly in a peripheral location within the liver.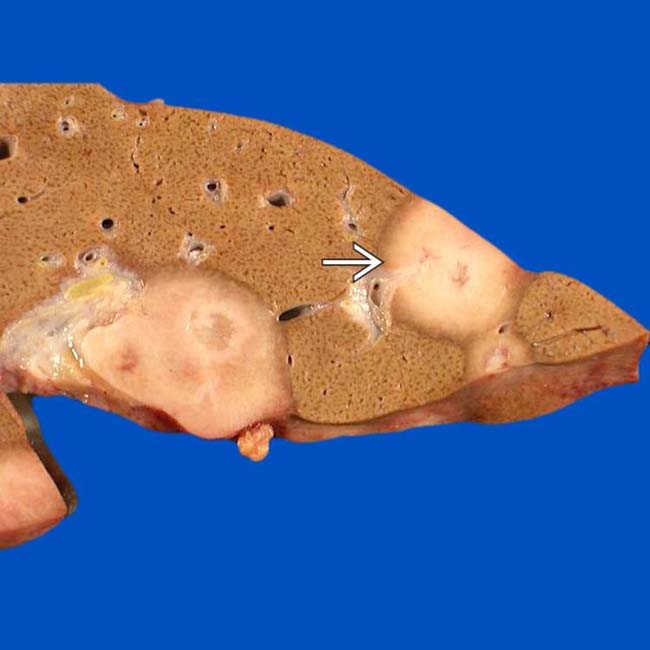
 and hyperemic tumor.
and hyperemic tumor.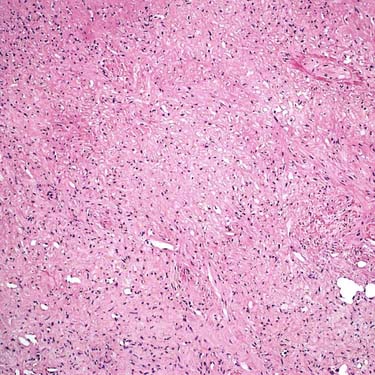



















 Tumor nodules show varied echogenicity pattern
Tumor nodules show varied echogenicity pattern





