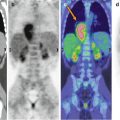
Fig. 34.1
Maximum intensity projection (a) shows abnormal 18F-FDG mediastinal uptake. Note the absence of pathological uptake in the bilateral cervical lymph nodes detected clinically, and the absence of FDG accumulation in the testicles that corresponded to the ultrasound findings and the diffuse radiotracer uptake of the skeleton probably of functional meaning. (b) CT and PET/CT fusion transaxial images display intense FDG accumulation in the anterior mediastinum
Teaching Point
18F-FDG–PET/CT evaluates molecular and functional changes and is therefore a valuable tool not only in the determination of the various possible causes of FUO but also in the detection of otherwise occult tumors or atypical infection.
References
1.
Petersdorf RG, Beeson PB (1961) Fever of unexplained origin: report on 100 cases. Medicine (Baltimore) 40:1–30CrossRef
2.
Durack DT, Street AC (1991) Fever of unknow origin-reexamined and redefined. Curr Clin Top Infect Dis 11:35–51PubMed
3.
Meller J, Sahlmann CO, Gürocak O, Liersch T, Meller B (2009) FDG-PET in patients with fever of unknown origin: the importance of diagnosing large vessel vasculitis. Q J Nucl Med Mol Imaging 53(1):51–63. ReviewPubMed
4.
Bleeker-Rovers CP, Corstens FH et al (2004) Fever of unknown origin: prospective comparison of diagnostic value of (18)F-FDG PET and (111)In-granulocyte scintigraphy. Eur J Nucl Med Mol Imaging 31:622–626CrossRef
5.
6.
Bleeker-Rovers CP, van der Meer JW, Oyen WJ (2009) Fever of unknown origin. Semin Nucl Med 39:81–87PubMedCrossRef
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


