Fig. 6.1
MDCT coronal reformatted image a shows a biliary stent (white arrows) migrated at the level of the pelvis. MDCT axial image b shows a fluid collection (white arrowheads) close to the biliary stent (white arrows)
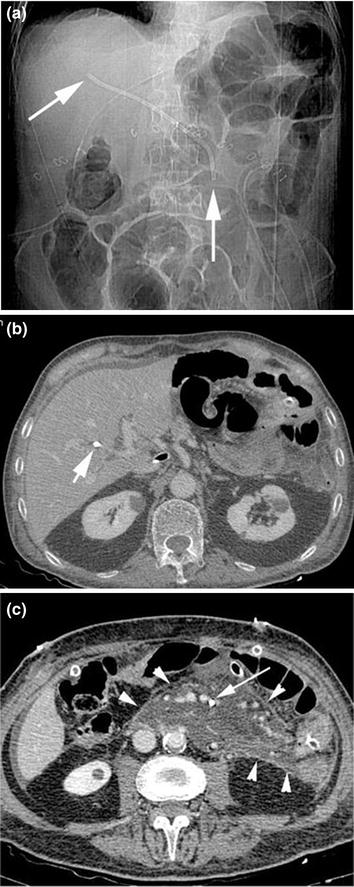
Fig. 6.2
Plain abdominal film a shows the presence of a biliary stent (white arrows): The distal tip of the stent is located in the left paravertebral side. MDCT axial image b demonstrates the proximal tip of the biliary stent (white arrow) located at the level of the left biliary duct. MDCT axial image c reveals the distal tip of the biliary stent (white arrow) located into the left mesenteric folds, surrounded by a large fluid collection (white arrowheads)
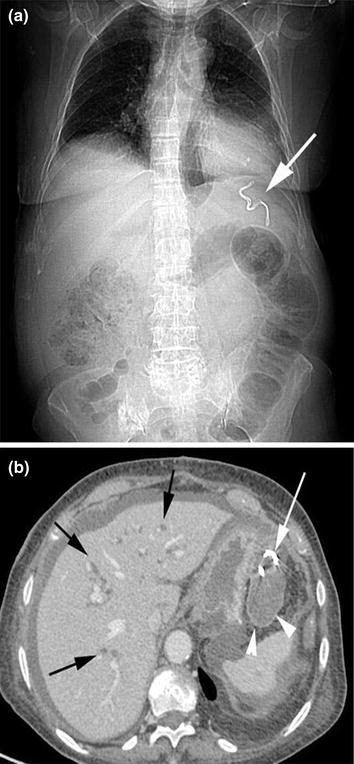
Fig. 6.3
MDCT, scout view a a biliary stent fragment (white arrow) is located in the left subphrenic space. MDCT, axial image b demonstrates the distal pigtail (white arrow) of the biliary stent located in the left subphrenic space, surrounded by a fluid collection (white arrowheads). The intrahepatic biliary system is enlarged (black arrows)
Known risk factors for distal migration include papillary stenosis, omission of sphincterotomy, use of plastic stents, and stenting of benign lesions. Patients with gastrointestinal symptoms with known stents should be meticulously worked up for the disease requiring stent placement, as well as for the risk of stent migration.
6.3 Gastrointestinal Stents
Gastrointestinal stents must be differentiated from other objects that may be found within the lumen of the gastrointestinal tract, as a result of a pathologic condition, e.g., bezoars (Fig. 6.4), swallowing of a diagnostic device (e.g., endoscopic capsules), or accidental or nonaccidental ingestion of some other object (e.g., batteries).
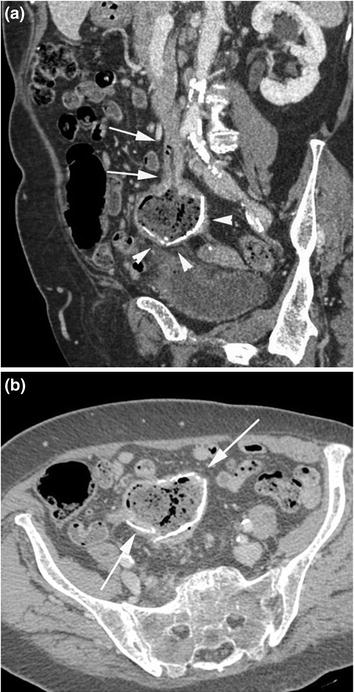
Fig. 6.4
MDCT oblique-coronal reformatted image a shows a calcified foreign body (phitobezoar) (white arrowheads) thrown out a small bowel loop (white arrows). MDCT axial image b reveals the calcified foreign body located in the mesenterial folds (white arrows)
In particular, ingestion of items of odontogenic origin (Fig. 6.5) by patients under general anesthesia or in elderly patients, including dislodged teeth, crowns, fixed partial dentures, and removable partial and complete dentures is not frequent but often goes unnoticed initially, leading to potentially dangerous late complications that require surgical intervention [14].
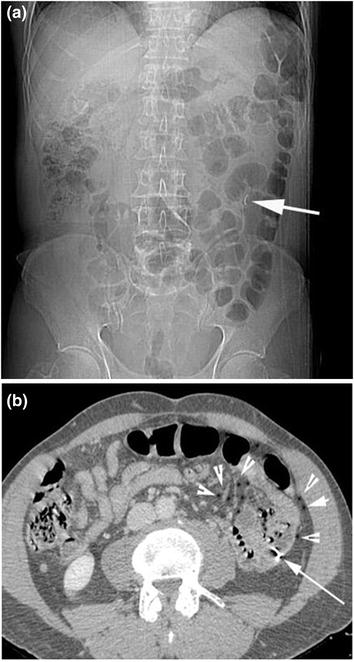
Fig. 6.5
Plain abdominal film a shows a metallic foreign body (dental-plate wire) in the lower left abdominal quadrant (white arrow). MDCT axial image b demonstrates the dental-plate wire blocked in the wall of a small bowel loop (white arrow). The loop has been perforated; there are some air bubbles spread in the near mesenterial folds (white arrowheads)
In the elderly population, especially in patients with dementia, dental prostheses appear to be the most commonly ingested foreign bodies in this population [15]. The main body of the prosthesis is usually made of acrylic resin, which is radiolucent, but they include radiopaque metallic clips and hooks [16]. Thus, many prostheses can be determined on plain radiographs.
Various dislodged tubes (Fig. 6.6) may be detected in the gastrointestinal tract: A tube should be recognized to establish that it no longer serves its intended purpose, and because it may mimic other swallowed foreign objects.
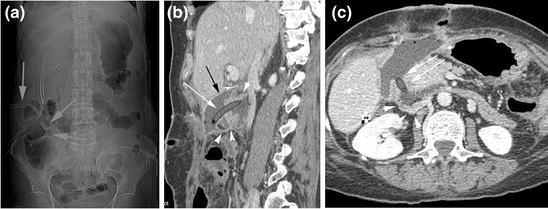
Fig. 6.6
Plain abdominal film a shows a transabdominal postoperation drainage tube (white arrows), located at the right lower abdominal quadrant. MDCT sagittal reformatted image b shows the drainage tube (white arrow) surrounded by a fluid collection (black arrow), passing through the duodenum inferior angle (white arrowheads). MDCT axial image c shows the drainage tube tip (white arrows) passing through the duodenum inferior angle (white arrowheads)
Complications of dislodged or forgotten tubes include penetration, perforation (Fig. 6.7), and obstruction of the wall of the intestine (Fig. 6.8).
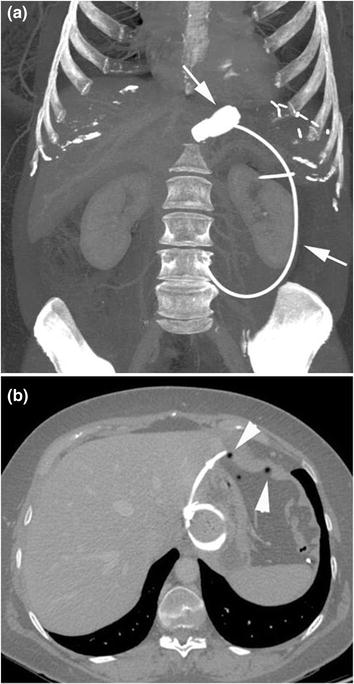
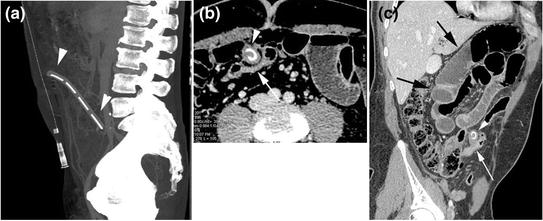
Fig. 6.7
MDCT, MIP coronal view a demonstrates a gastric bandage (white arrow). MDCT axial image b shows air bubbles entrapped in diaphragmatic tendons (white arrowheads), due to gastric bandage decubitus ulcer of the fundus
Fig. 6.8
MDCT, sagittal image a shows a surgical drainage tube forgotten in abdominal cavity (white arrowheads). MDCT axial image b demonstrates a fibrotic tissue around the tube (white arrowhead) joined to a closed small bowel loop (white arrow). MDCT oblique-coronal reformatted image c shows small bowel loops obstruction (black arrows), proximally to the closed small bowel loop (white arrow) and the tube (white arrowhead)
Stents used to overcome malignant biliary and gastrointestinal stenoses are made of plastic or metal. Stents to treat the latter, usually made of nitinol or stainless steel, can be bare, partially covered (at the center), or covered. The internal nonporous membrane prevents tumor growth through the mesh. Uncovered stents migrate less frequently, but they have significantly higher obstruction rates because of tumor ingrowth. Moreover, stents can be balloon expandable or, more frequently, self-expanding [17




Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
