Fig. 4.1
Gossipyboma: radiolucent material (surgical drape) is seen on left side (arrowheads)
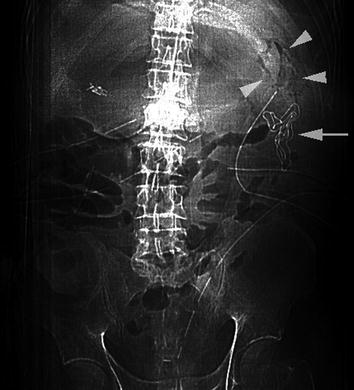
Fig. 4.2
Gossipyboma: radiolucent material (arrowhead) and radio-opaque marker (arrow) are seen on upper left side after splenectomy
The advantage of this technique, in suspected sponge forgetting in abdominal cavity, is related to the possibility to perform the investigation immediately after surgery with a portable X-ray machine, when the patient is still in the operating theater under anesthesia.
If gossipyboma has resulted in fistula formation, oral contrast may be administrated to help in its identification and thus the correct diagnosis [15].
Displaced abdominal wall meshes is a rare event, linked to the occurrence of complications after surgery. In most cases, only the staples that fix the mesh to the abdominal fascia are seen with plain abdominal radiography (Fig. 4.3) [7].

Fig. 4.3
Plain abdominal radiograph in a patient with incisional hernia repair. Only the staples (arrowhead) that fix the mesh to the abdominal fascia are seen with this technique
Usually indeed, the mesh is translucent and does not appear visible. In addition, this technique does not show accurately the presence of complications.
US
A surgical sponge retained in the abdominal cavity can often be detected sonographically. Its characteristic appearance is a well-delineated and hyper-reflective lesion with wavy internal echo, strong posterior shadow, and hypoecoic ring [16]. At ultrasound images we recognize sponges as cystic or solid type mass. The former consist of a cystic lesion with a winding echogenic bundle, and the latter as a complex structured mass with hyper and hypoechoic areas (Fig. 4.4) [17].
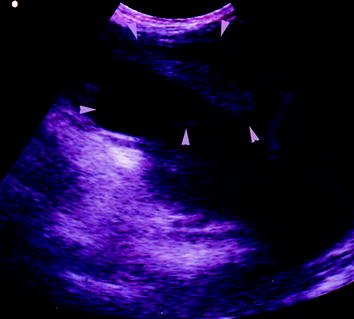
Fig. 4.4
An abdominal mass of complex structure (gossipyboma) adherent to the anterior peritoneum
The pattern of acoustic shadowing changes with the direction of the ultrasound beam but is caused by material itself, indicating calcified regions or a pocket of air. The sonographic detection of a mass with high echoes casting acoustic shadows should alert radiologists to the likelihood of retained surgical sponges.
Abdominal wall meshes on ultrasound appear as hyperechoic lines. Sonographically, we can identify postoperative complication as fluid collection and we can differentiate between hematoma or seroma (Fig. 4.5). In some cases, especially those in which septa or air is noted inside the collection, it is difficult to make the distinction.
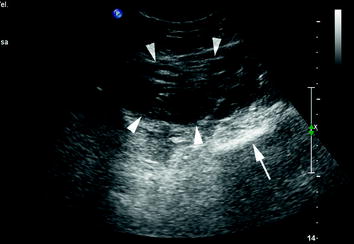
Fig. 4.5
Abdominal wall e-PTFE mesh seen as hyperechoic lines (arrow) displaced by hematoma (arrowheads)
Also, purulent collection around the mesh and bowel complication due to adhesion or mesh displacement is identified by ultrasound easily [17].
Displacement only without complications is not identifiable by ultrasound.
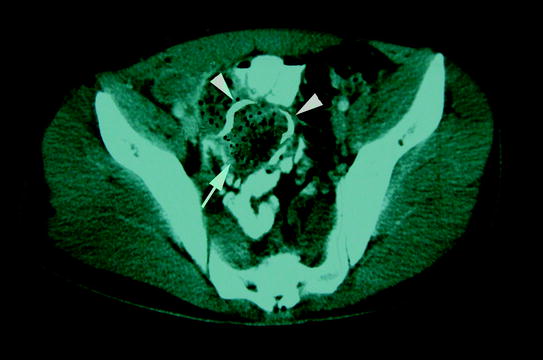
CT
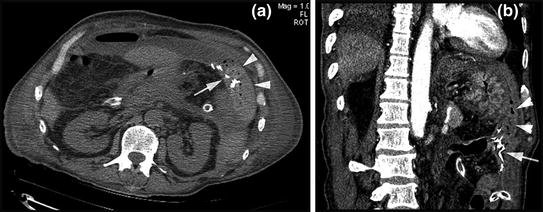
Gossipyboma and their possible complications are best identified on CT. Most authors describe well-circumscribed disomogeneus masses with a thick wall, often with gas bubbles inside, sometimes without showing calcification or wall enhancement after administration of i.v. contrast medium (Fig. 4.6a, b) [14]. The internal structure of such masses may be whirl-like or spongiform due to gas-trapped bubbles in the sponge. It may be of low density or complex, with both low density and wavy, striped or spotted high-density areas (Fig. 4.7) [18]. The radio-opaque marker strip is of a thin metallic density in the mass (Fig. 4.8a, b).
 Foreign Bodies as Complications of Endovascular Devices
Foreign Bodies as Complications of Endovascular Devices
 Plain Film and MDCT Assessment of Neck Foreign Bodies
Plain Film and MDCT Assessment of Neck Foreign Bodies
 Foreign Bodies of the Gastrointestinal Tract
Foreign Bodies of the Gastrointestinal Tract
 Foreign Bodies and Penetrating Injuries
Foreign Bodies and Penetrating Injuries
 Foreign Bodies as Complications of Biliary Stents and Gastrointestinal Stents
Foreign Bodies as Complications of Biliary Stents and Gastrointestinal Stents
 Tracheobronchial Foreign Bodies
Tracheobronchial Foreign Bodies




Fig. 4.6
The same case as in Fig. 4.2a, b Gossipyboma in upper left side, with a spongiform pattern (arrowheads) and radio-opaque marker (arrows)
Related posts:
Foreign Bodies as Complications of Endovascular Devices
Plain Film and MDCT Assessment of Neck Foreign Bodies
Foreign Bodies of the Gastrointestinal Tract
Foreign Bodies and Penetrating Injuries
Foreign Bodies as Complications of Biliary Stents and Gastrointestinal Stents
Tracheobronchial Foreign Bodies
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
