Fig. 2.1
Radiopaque foreign body (stud earring) in right main bronchus

Fig. 2.2
Radiopaque foreign body (stud earring)

Fig. 2.3
Stud earring bronchoscopically removed

Fig. 2.4
Inspiratory chest radiograph. No evidence of radiopaque foreign body. Hyperinflation of right lung
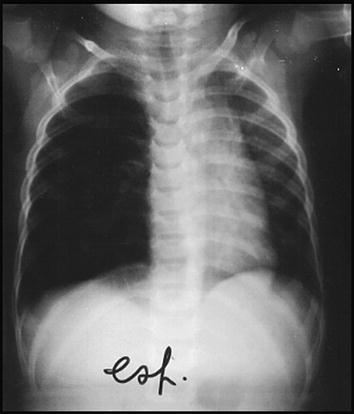
Fig. 2.5
Expiratory chest radiograph: air trapping in the right lung with contralateral mediastinal shift
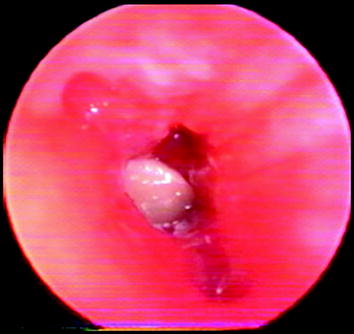
Fig. 2.6
At bronchoscopy food particle obstructing right main bronchus
When entering in the lower respiratory tract larger and heavier material or fluid should follow the straightest and most gravitary course and should preferentially locate in the right main-stem bronchus or in the right lower bronchus with axis angulated at only 20–30° with respect to the tracheal one compared to 40–60° of the left main stem bronchus’ axis.
Indeed, preferential location of tracheobronchial foreign body in the right bronchial tree was demonstrated only for the adult population of a study comparing a child and adult patient population. Moreover, in the child group, foreign bodies were preferentially found in the proximal airways (larynx, trachea, and right and left main bronchi) probably because of their minor caliber [1].
When reaching the lung, finer and more fluid materials preferentially involve, in the supine position, the dependent posterior segments of the upper lobe, and the apical segments of the lower lobe.
In orthostatism, there is the preferential involvement of the basilar segments of the lower lobes and localization is more diffuse as in other areas of the lung (Figs. 2.7, 2.8, 2.9, and 2.10).
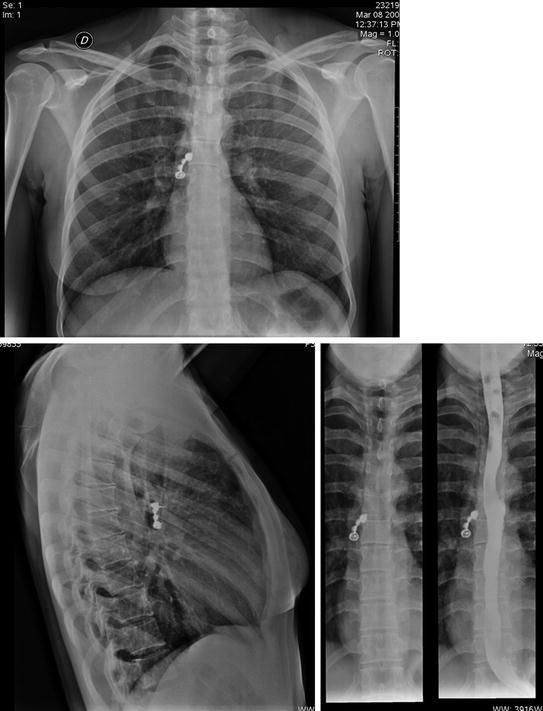
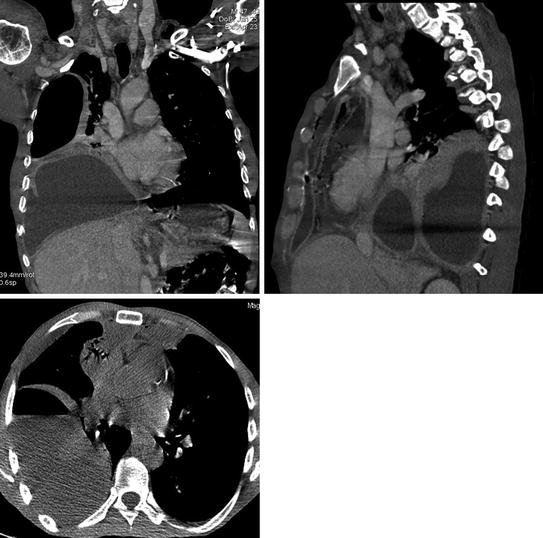

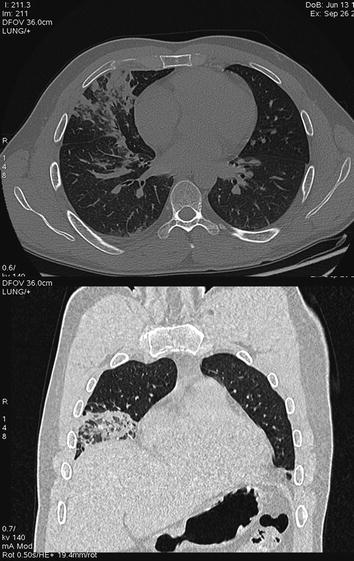
Fig. 2.7
Radiopaque dental bridge (four elements) projecting in the right main bronchus
Fig. 2.8
CT performed for mediastinitis in patient with odontogenous abscess. Calcific opacity in the lumen of a segmental bronchi of right lower lobe suspected for foreign body. At bronchoscopy removal of fragment of tooth in B8
Fig. 2.9
Wisthler lodging in the left main bronchus (endoscopically removed)
Fig. 2.10
Accidental aspiration of gasoline
In the lateral decubitus, the distribution regards preferentially the apical and posterior upper lobe.
The anterior portions of the lung are usually involved when aspiration occurs in the prone position, as in near-drowning.
Aspirated material can come not only from external sources but also from inner sources: such as from esophagus or stomach in situations of functional or anatomical defects (tracheobronchial-fistulas). Infective foci of the nasal, oropharyngeal cavity or of the lung itself (cyst or abscess fluid-filled or tubercular cavity) can become another source of aspirate.
A little amount of aspiration of oral or gastric secretions is considered frequent during sleep and anesthesia also in normal adults and is usually not clinically significant.
Nasopharyngeal and oropharyngeal tubes for endoscopy or tracheostomy do not prevent but actually increase the risk of aspiration.
Most frequent aspirated particles are piece of food (nuts, legumens, seeds, fragments of animal bones) and teeth, or little objects or pieces of toys.
The effects of aspiration depend on the amount of aspirated material, the dimensions of the particles, and their chemical nature; they can be acute or chronic.
The nature of aspirate can produce different aspiration syndromes:
GASTRIC ACID Acute, massive aspiration of a great amount of gastric acid (pH less than 2.5) is called Mendelson’s syndrome and determines in a few minutes an acute chemical lung injury with severe alveolar damage defined as Aspiration Pneumonitis.
Chronic repeated aspiration of small quantities of gastric acid is involved in recurrent pneumonia and chronic fibrosis.
PARTIALLY DIGESTED FOOD and in particular lentils and other leguminous material such as beans and peas can cause a granulomatous pneumonitis called lentil aspiration pneumonia.
INFECTIOUS MATERIAL from the oropharinx, especially in patients with poor oral hygiene and advanced periodontal disease, can cause an infectious process called Aspiration Pneumonia.
WATER, fresh or salt, when aspirated in great quantity in near-drowning cause pulmonary edema.
SAND or GRAVEL may be aspirated during drownings, surfing accidents, and motor vehicle collisions.
LIGTHER HYDROCARBONS can be aspirated from a person who has siphoned fuel and from fire-eaters.
If aspirated in great quantity they cause a chemical pneumonia called fire-eater pneumonia.
OIL ASPIRATION mineral oil and oily nose drops cause exogenous lipoid pneumonia.
BARIUM ASPIRATION may occur during imaging of the gastrointestinal tract (Fig. 2.11), [3, 4].

Fig. 2.11
Alveolar hyperdensities from pregressed aspiration of barium
Related posts:
 Foreign Bodies as Complications of Endovascular Devices
Foreign Bodies as Complications of Endovascular Devices
 Plain Film and MDCT Assessment of Neck Foreign Bodies
Plain Film and MDCT Assessment of Neck Foreign Bodies
 Foreign Bodies of the Gastrointestinal Tract
Foreign Bodies of the Gastrointestinal Tract
 Foreign Bodies and Penetrating Injuries
Foreign Bodies and Penetrating Injuries
 Foreign Bodies as Complications of Biliary Stents and Gastrointestinal Stents
Foreign Bodies as Complications of Biliary Stents and Gastrointestinal Stents
 Intra-Abdominal Foreign Bodies: Gossypiboma and Abdominal Wall Meshes
Intra-Abdominal Foreign Bodies: Gossypiboma and Abdominal Wall Meshes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


