Fig. 17.1
Large ganglion adjacent to the radiocarpal joint. Ultrasonography discloses the presence of an anechoic mass with well-defined margins, which is in contact with the extensor digitorum communis and extensor indicis proprius tendons (Est cd pi). During flexion and extension of the wrist (a, b), the mass impinges on the two tendons, causing tenosynovitis (b)
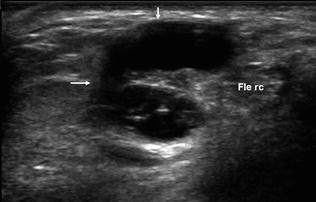
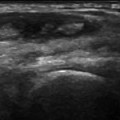
Fig. 17.2
Ganglion with atypical features on ultrasound in contact with the radiocarpal joint. Ultrasonography reveals a multiloculated anechoic cyst-like mass surrounding the flexor carpi radialis tendon (Fle rc). At this level, the lesion has to be differentiated from flexor carpi radialis tenosynovitis
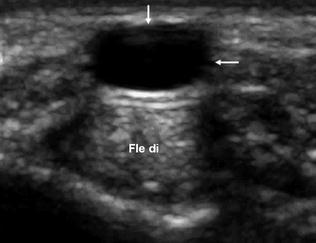
Fig. 17.3
Ganglion in contact with the A1 pulley. The sonographic examination reveals an anechoic mass with well-defined margins superficial to the flexor digitorum superficialis and profundus tendons (Fle di). On dynamic studies, a ganglion that is in contact with a flexor tendon sheath will move with the sheath when the fingers are flexed. In this case, the ganglion was in contact with the A1 pulley (which does not move during flexion of the fingers), so the lesion did not move during flexion
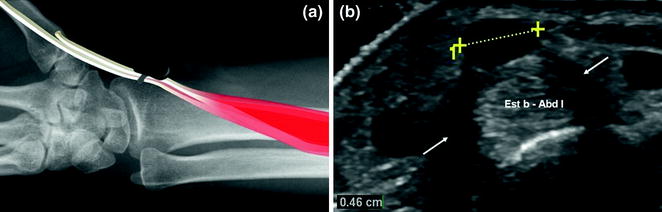
Fig. 17.4
Ganglion in contact with the retinaculum of the first dorsal compartment (a). The sonographic study shows a well-defined anechoic mass butting against the retinaculum of the first osseofibrous tunnel (b) (arrows). The diagnosis is confirmed when the thumb is flexed and extended: the tendon and tendon sheath move freely, whereas the retinaculum and the adjacent ganglion remain where they are
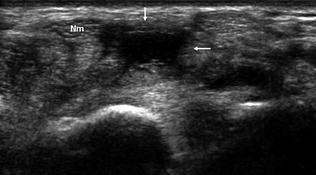
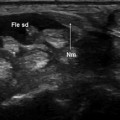
Fig. 17.5
Ganglion inside the carpal tunnel. The patient had electromyographically diagnosed carpal tunnel syndrome. The sonographic examination reveals the presence of a ganglion cyst (arrows




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
