Stomach rotates upward, with greater curvature lying above lesser curve
• Mesenteroaxial volvulus: Rotation of stomach about its short axis
More common type in children
• Entire stomach may be herniated (type IV paraesophageal hernia [PEH]) or only part (type III PEH)
Either can result in volvulus ± obstruction ± ischemia
Gastric wall pneumatosis indicates ischemia
• Diagnosed with upper GI &/or CT
• CT is better at demonstrating associated hernias and gastric ischemia
TOP DIFFERENTIAL DIAGNOSES
• Hiatal hernia
Types III and IV PEHs increase risk for gastric volvulus
• Postoperative state, stomach
Esophagectomy with gastric pull through (conduit may twist and obstruct)
• Epiphrenic diverticulum
CLINICAL ISSUES
• Treatment: Open or laparoscopic detorsion and gastropexy
DIAGNOSTIC CHECKLIST
• Presence or absence of obstruction and ischemia are more important than remembering or reporting whether volvulus is organo- or mesenteroaxial
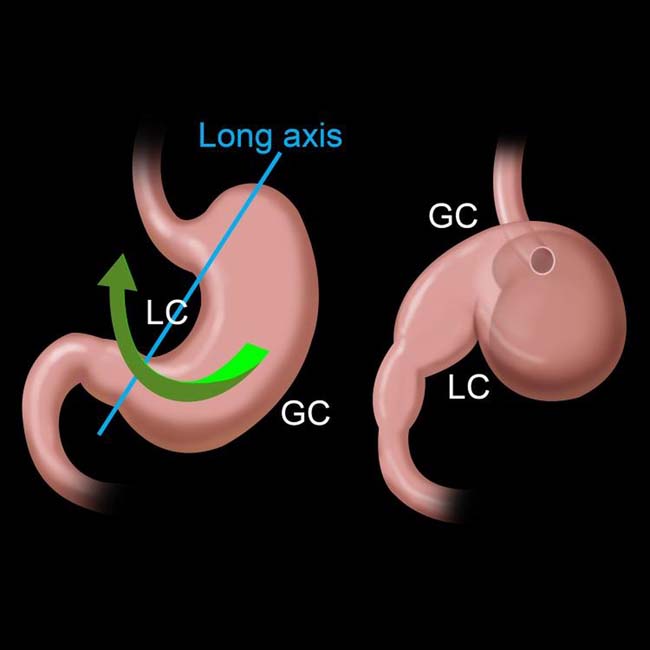
(Left) Graphic illustrates an organoaxial gastric volvulus, in which the stomach twists along its long axis, resulting in the greater curvature (GC) lying above the lesser curvature (LC).
(Right) Film from an upper GI series in a 73-year-old woman shows a type IV paraesophageal hernia (PEH) with organoaxial volvulus but little or no obstruction. The greater curvature of the stomach lies above the lesser curvature. The small bowel is also herniated through a large diaphragmatic defect.
(Left) Axial CECT demonstrates an intrathoracic stomach (type IV PEH) in a 81-year-old woman with mild chest pain and a known brain malignancy. The stomach is dilated with 2 air-fluid levels, indicating obstruction.
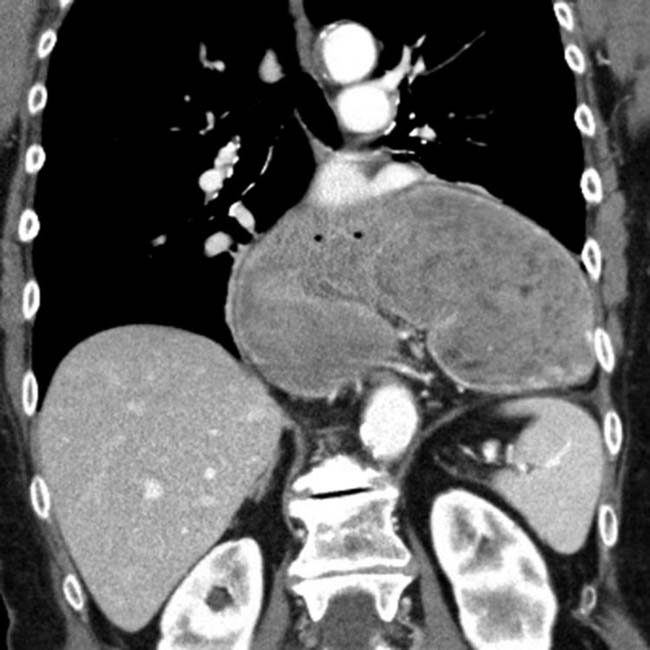
(Right) Coronal CECT in the same patient demonstrates an “upside-down” configuration of the stomach, with reversal of the greater and lesser curvatures, in keeping with an organoaxial volvulus.
TERMINOLOGY
Abbreviations
• Gastric volvulus
Definitions
• Uncommon acquired twist of stomach on itself
IMAGING
General Features
• Morphology
Abnormal degree of rotation of 1 part of stomach around another part
• Types of volvulus: Organoaxial (most common), mesenteroaxial, mixed
• Organoaxial volvulus: Rotation of stomach around its longitudinal axis
Around line extending from cardia to pylorus
Stomach rotates upward, with greater curvature lying above lesser curvature
Antrum moves from inferior to superior position; fundus rotates superior to inferior
Usual setting is with a large paraesophageal hernia (PEH)
– Type III PEH = Gastroesophageal (GE) junction and portions of fundus and body herniate into chest
– Type IV PEH = GE junction and almost entire stomach lie within chest
• Mesenteroaxial volvulus: Rotation of stomach about its mesenteric (short) axis
Axis running transversely across stomach at right angles to lesser and greater curvatures
Stomach rotates from right to left, or left to right about long axis of gastrohepatic omentum
Not necessarily in setting of hiatal hernia
May result from congenital absence or laxity of gastric ligaments
• Mixed volvulus: Combination of organoaxial and mesenteroaxial volvulus
Radiographic Findings
• Radiography
Abdominal plain films; patient upright
– Double air-fluid level
– Large, distended stomach; seen as air- and fluid-filled spheric viscus displaced upward and to left
– Small bowel collapsed if stomach is obstructed
Chest film: Intrathoracic; upside-down stomach
– Retrocardiac fluid level; 2 air-fluid interfaces at different heights; suggests intrathoracic gastric volvulus
Fluoroscopic Findings
• Upper GI
Massively distended stomach in left upper quadrant extending into chest
Inversion of stomach (upside-down stomach)
– Greater curvature above level of lesser curvature
– Positioning of cardia and pylorus at same level
– Downward pointing of pylorus and duodenum
Volvulus with > 180° twist causes luminal obstruction
Incomplete or absent entrance of contrast material into &/or out of stomach; acute obstructive volvulus
May see “beaking” at point of twist
Mesenteroaxial: Antrum and pylorus lie above gastric fundus
CT Findings
• CT appearance may be variable
Depends upon extent of gastric herniation, points of torsion and final positioning of stomach
May see linear septum within gastric lumen; corresponding to area of torsion
• Entire stomach may be herniated (type IV PEH) or only part (type III PEH)
Either can result in volvulus ± obstruction ± ischemia
Ischemia seen as lack of contrast enhancement of gastric wall ± pneumatosis within wall
• CT chest and abdomen; performed preoperatively
To detect associated malformation or malposition and site, size, level of diaphragmatic defect
MR Findings
• Coronal images demonstrate 2 points of twisting
Different signal intensities reflect point of torsion
Angiographic Findings
• GV may present as acute upper gastrointestinal hemorrhage
Imaging Recommendations
• Best imaging tool
Upper GI series
– Demonstrates focus of twist; anatomic detail
Only gold members can continue reading. Log In or Register to continue







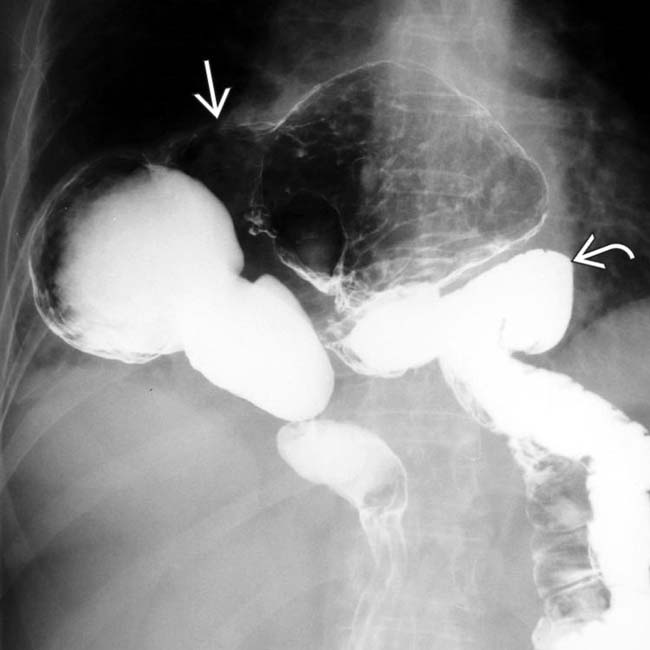
 lies above the lesser curvature. The small bowel
lies above the lesser curvature. The small bowel  is also herniated through a large diaphragmatic defect.
is also herniated through a large diaphragmatic defect.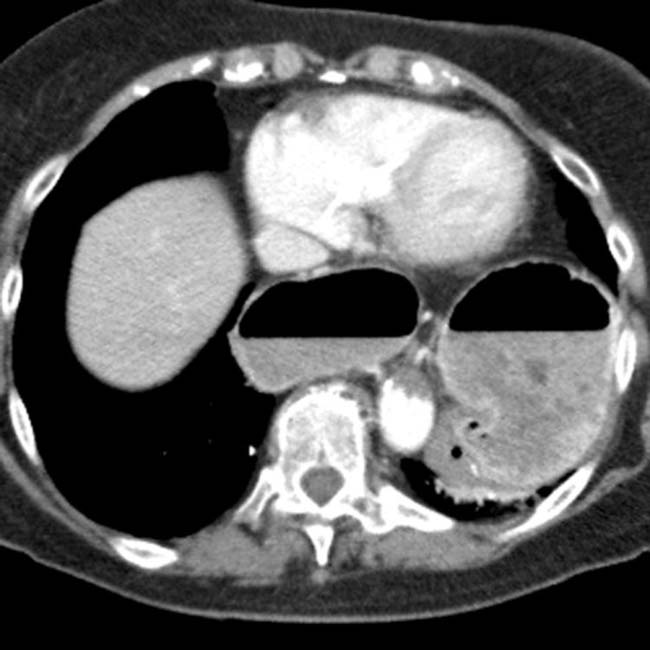























 Upper GI series
Upper GI series





