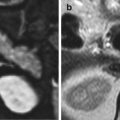
Fig. 8.1
Anatomy of the esophagus (E), frontal (a) and left-lateral projections (b). The connection with the aorta (Ao) is highlighted, and we can see the vertebral bodies and the trachea (T), marked in (a). GEJ gastroesophageal junction
The lumen, at rest, is a star-shaped virtual cavity, and such a shape is due to the longitudinal folds of the mucosa and submucosa layers; it becomes an actual cavity after the passage of the alimentary bolus.
The esophagus has three curves, one of them on the sagittal plane and two on the frontal plane, slightly on the left compared to the medial axis. It descends beside the anterior spinal convexity, down to the fourth thoracic vertebra, slightly on the left of the median axis; subsequently, it detaches from the column, with a posterior convex curve; it crosses the aortic arch, with a first smooth curve, convex toward the right side, and immediately below, it forms a second sharper curve toward the left.
Along the course of the esophagus, we can distinguish four points of constriction: the cricoid constriction (at the origin), the aortic and bronchial constriction (respectively at the crossing point with the aortic arch and the main bronchus), and the diaphragmatic one. The segments between them are called, respectively, cricoid-aortic, broncho-diaphragmatic, and precordial segments.
The esophagus can be divided into four parts: the cervical, thoracic, diaphragmatic, and abdominal parts.
The cervical portion is about 4–5 cm long, located deeply inside the neck, and originates from the pharynx (esophageal ostium or Killian ostium) at the level of the sixth cervical vertebra, up to the superior margin of the second thoracic vertebra. Anteriorly, it is connected to the membrane of the trachea by soft connective tissue and by the tracheoesophageal muscular tissues. There is only a free part on the anterior face of the esophagus, which is in connection with the left thyroid lobe, the left recurrent laryngeal nerve, and the sternohyoid and sternothyroid muscles. It is also connected: posteriorly, through the interposition of the retroesophageal space (direct continuation of the retropharyngeal one), to the deep cervical fascia, and, through the same, to the spinal column, and laterally, with the right and left common carotid arteries and, on the right, with the recurrent laryngeal nerve.
The thoracic portion, 16 cm long, is located in the posterior mediastinum from the second thoracic vertebra to the diaphragm, further divided into two tracts when it crosses the main left bronchus: the first one, the epibranchial tract, is anteriorly connected to the trachea and the initial part of the main left bronchus, to which is strictly attached by means of the bronchoesophageal muscle; posteriorly, to the spinal column (up to the fourth thoracic vertebra); and laterally, on the right side, to the mediastinal pleura (forming the azygo-oesophageal recess) and, on the left side, to the mediastinal pleura, the aortic arch, and the initial tract of the descending aorta. The second tract, called hypobranchial, is connected, anteriorly, to the posterior part of the pericardium that covers the left atrium and with the lymph nodes of the tracheobronchial bifurcation and, laterally, to the vagus nerves.
The diaphragmatic portion, about 1–2 cm long, is connected to the esophageal hiatus, anterior to the aortic orifice; a small muscle may originate from the diaphragm, the so-called phrenicoesophageal muscle. However, the esophagus is attached to diaphragm by the phrenicoesophageal ligament (this collagenous band tends to weaken and elongate with age and may lead to hiatal hernia).
Lastly, the abdominal portion, about 3 cm long, forms an acute angle with the gastric wall (angle of His) and opens up on the bottom of the stomach, and it is named cardia. It is anteriorly related with the posterior face of the left hepatic lobe, and posteriorly with the abdominal aorta and the medial diaphragmatic pillars, on the right side with the hepatic caudate lobe and on the left with the bottom of the stomach.
The union of the diaphragmatic (epiphrenic) and the abdominal tracts is termed gastroesophageal vestibule.
The esophagus, a cave tubular organ, is composed of four layers: tunica mucosa, tela submucosa, tunica muscularis, and the tunica adventitia. It is supplied by the inferior thyroid arteries (cervical portion), bronchial and esophageal branches of the aorta (thoracic tract), esophageal branches of the aorta, and the left gastric and phrenic arteries (diaphragmatic and abdominal part). The refluent blood is drained into the submucosa layer of the esophagus and, subsequently, into the tributary periesophageal plexus, from where the esophageal veins, flowing into the azygos vein, originate; some other veins drain into the hemiazygos and accessory hemiazygos vein and into the anterior and posterior intercostal veins (lateral branches of the hemiazygos and azygos one) following the course of the ribs. The veins included in the cervical part of the esophagus merge into the inferior thyroid vein, and the abdominal ones into the left gastric vein, and drain into the portal vein.
The lymphatic system drains into the periesophageal lymph nodes (deep cervical, paratracheal, posterior mediastinal, and superior gastric lymph nodes).
Innervation is supplied by the esophageal plexus, consisting of the sympathetic and parasympathetic branches of the vagus nerve.
8.1.2 Stomach
The stomach is an organ of the digestive system responsible for the second phase of the digestion, which follows the chewing phase; it is a flattened sac, topographically located in the region of the left hypochondrium and epigastrium; its major axis is vertical in the long-limbed subject, while it is mainly horizontal in the short-statured one. It consists of an anterior and posterior face, a concave right margin (the lesser curvature), and a left convex one (the greater curvature) (Fig. 8.2).
Fig. 8.2
Gastric cavity, longitudinal section along the two curvatures. Fundus, body, and antrum, respectively, star, triangle, and circle. The arrow is on the gastroesophageal junction, the arrowhead on the duodenum. Ao aorta, E esophagus
The lesser curvature is the posterosuperior margin of the stomach; it is oriented toward the right and inferiorly, then, at the level of the angular incisure; it softly turns upward and descends again, terminating at the level of the pylorus. This is the insertion point of the hepatogastric ligament which connects the liver and the stomach; the subsequent tract is termed hepatoduodenal ligament and coincides with the lesser omentum.
The greater curvature is four–five times longer than the lesser one; it originates at the level of the cardiac notch, and it turns upward forming the dome-shaped margin of the gastric fundus; starting from the highest point, it subsequently goes downward and medially up to the intermediate sulcus that separates the antrum from the pyloric canal. It is covered with peritoneum; laterally, the two peritoneal visceral sheets (anterior and posterior) merge into the gastrosplenic ligament, which connects the wall of the stomach to the splenic hilum; posteriorly, the greater curvature is next to the body and tail of the pancreas and to a portion of the left hepatic lobe. The gastrocolic ligament goes from the greater curvature to the transverse colon, the right colic flexure, and the duodenum, coinciding with the anterior root of the greater omentum.
The anterior surface (superior) of the stomach is covered with peritoneum and adjacent to the diaphragm, the spleen (determining its gastric face), part of the left hepatic lobe and of the quadrate lobe, and the transverse colon. The posterior surface (inferior) of the stomach is connected to the left suprarenal (adrenal) gland, body and tail of the pancreas, aorta, lienal and hepatic arteries, and portal vein; it is completely covered with peritoneum, with the exception of the part closer to the cardia, which touches the diaphragm.
There are two orifices in the stomach (cardia and pylorus) and four main portions (bottom, body, pyloric antrum, and pyloric canal).
The cardia connects the stomach to the esophagus, it is not covered with peritoneum, and the tunica muscularis is not thickened; it allows the passage of the alimentary bolus in craniocaudal direction only: the esophageal reflux is prevented by the muscular tone and by the oblique fibers of the internal tunica muscularis, forming a virtual valve for the closure of the lumen. The border between stomach and esophagus is the Z line, a squamous or columnar structure, consisting of gastric mucosa, which slightly enters into the esophageal lumen and terminates with a “zigzag” profile. The mucosa of the cardia is characterized by typical reliefs called “mucosal rosette,” which are involved in the prevention of the gastroesophageal reflux.
The fundus, touching posteriorly the diaphragm, is a vault above an imaginary horizontal line starting from the cardiac notch; from the radiological point of view, it coincides with the gastric bubble, the air-filled part of the stomach, and therefore radiotransparent. Its projection on the thoracic wall is called semilunar Traube’s space, delimited, below, by the inferior margin of the ninth costal cartilage and the xiphoid process of the sternum; above, by the fifth and sixth ribs; and laterally, on the left side, by the costal arch and, on the right side, by the anterior margin of the liver. The mucosa on the gastric fundus forms some temporary folds that flatten when such an organ is relaxed.
The body is the bigger part of the stomach: it is a cavity, narrowed inferiorly and with vertical axis, slightly tilted on the left; it is included between the bottom and the angular incisure. The mucosa forms redundant permanent folds (rugae), more visible in posteromedial, medial, and anteromedial regions and therefore next to the lesser curvature. The folds are more wrinkled on the internal walls of the greater curvature, progressively more defined toward the bottom, at the border with the antrum. The latter has a cylindrical shape; it is above the body, lateral, between the angular incisure and the intermediate sulcus. The mucosa is mainly smooth; during contraction, however, some remarkable, longitudinal folds appear next to the pyloric canal; they are more similar to those of the lesser curvature rather than those of the greater one.
The pyloric canal, inferior and lateral to the pyloric antrum, is the hemispheric portion between the intermediate sulcus and the pylorus. The latter is the muscular sphincter between the stomach and the duodenum; it can be located on the basis of the point of constriction of the pyloric canal; it consists of smooth circular muscular fibers, thickened and woven with other oblique fibers.
In men, the capacity of the stomach is around 1 l, when empty; after normal meals, it generally expands in order to collect almost one liter of alimentary bolus, but it can contain up to 4 l; in such events, the enlargement determines compression of the other organs contained in the abdominal and thoracic cavity. Gas deriving from the digestion tends to go up and concentrate on the gastric fundus, which represents the superior portion of the organ (gastric bubble).
The gastric walls, such as the intestine ones, are divided into four layers: mucosa, submucosa, muscular, and serous tunicae.
The main gastric arteries and the numerous anatomical variants originate from the celiac trunk that ramifies into the lienal artery (on the left), the gastric artery (above), and the common hepatic artery (on the right). The veins mainly drain into the portal vein and the lienal and the superior mesenteric veins; the venous distribution may vary.
The lymph vessels of the stomach are part of the dense network contained in the superior part of the abdominal cavity; in particular, they continue from the esophageal and duodenal systems, but also from the pancreatic, hepatic, and splenic ones. There are three different systems: the first one drains the superior part of the anterior and posterior faces of the gastric fundus and body, of the antrum, and the pyloric canal, and from there, into the celiac lymph nodes; the second one drains the inferior part of the anterior and posterior surfaces of the body, of the antrum, and pyloric canal, flowing into the subpyloric and gastroepiploic lymph nodes on the right side; finally, the lymph coming from the left inferior part of the body, and from the left side of the fundus, flows into the gastroepiploic lymph nodes, which drain the lienal nodes. The lymph of the stomach flows into the receptaculum chyli (or cisterna chyli), through the celiac lymph nodes.
The sympathetic innervation of the stomach originates from the celiac and hepatic plexuses, the major and minor splanchnic nerves, corresponding to the anterior branches of the thoracic nerves from the fifth to the twelfth vertebral body; their main functions are vasoconstriction, inhibition of the gastric muscles, and stimulation of the pyloric contraction. The sympathetic nerve branches, originating from the celiac plexus, are mainly sent to the posterior (inferior) surface of the antrum and the stomach, the branches arriving from the hepatic plexus to the anterior (superior) surface and to the fundus. The parasympathetic innervation of the stomach originates from the branches of the anterior and posterior vagus nerves.
8.1.3 Small Intestine
The small intestine is the longest segment of the digestive canal; it is 6–8 m long (with a high individual variability from 2.5 to 11 m), located from the pyloric sphincter to the ileocecal valve, through which it enters the large intestine. It looks like a cylindrical tube with several curves, going from the epigastrium to the right iliac fossa; it occupies most of the abdominal cavities and pelvis cavities (Fig. 8.3). Its capacity is approximately 6 l and its diameter progressively reduces in proximal to distal direction from 4.7 to 2.7 cm. The small intestine has a double function: the first tract is responsible for food digestion, while the second tract for the absorption of digestive products. More precisely, we can distinguish a proximal portion, the duodenum, about 30 cm long, and a distal portion, the small bowel, conventionally divided into jejunum and ileum. This part is included in the free margin of a large fan-shaped peritoneal fold, called mesentery, originating from the posterior part of the abdominal cavity and reaching the anterior margin of the intestinal canal: such an anchoring allows great mobility of the jejunum-ileum tract.
Fig. 8.3
Morphology and location of the small bowel. The stars are on the mesentery; the arrowheads show one of the three taeniae of colon. AC ascending colon, C cecum, D duodenum, HF hepatic flexure, SF splenic flexure, TC transverse colon
8.1.3.1 Duodenum
The duodenum is the first of the three segments of the small intestine; it is more static compared to the other two portions (jejunum and ileum), characterized by higher mobility. It collects the bile from the choledochus and the pancreatic juice from the pancreatic duct of Wirsung through the major duodenal papilla (of Vater), fitted with the sphincter of Oddi; it also neutralizes the acidity of the gastric chyme through the alkaline secretion of the Brunner’s glands, typical of the structure of this part of the small intestine.
The duodenum, with an average length of 20–25 cm, originates from the pylorus and surrounds, with its typical C shape, the head of the pancreas; with the exception of the first 2.5 cm, it is a retroperitoneal organ, attached to the posterior walls of the abdominal cavity.
It consists of four parts: superior, descending, horizontal, and ascending part.
The triangular first part (bulb) has a greater movement capacity; it consists of a cylindrical tube originating from the pylorus; it later moves on the right, along the medal line, and posterolaterally for about 5 cm, ending into the superior flexure (knee). The visceral peritoneum covers the anterior and superior-posterior faces, contributing to the formation of the anterior wall of the epiploic foramen (foramen of Winslow). On the superior margin, we find the insertion of the hepatoduodenal ligament, which represents the pars tensa of the lesser omentum; the superior margin of the greater omentum is partly attached to the inferior margin. The peritoneum covers only the anterior face of the terminal first portion, which is related, anteriorly, to the right hepatic lobe and the gallbladder; inferiorly, to the head of the pancreas; and, posteriorly, with the abdominal wall and the medial margin of the right kidney.
The descending part (second part) of duodenum is a vertical, cylindrical tube located in the submesocolic cavity. It is a direct continuation of the first part, through the superior knee, and continues in the horizontal part, through the right duodenal flexure or inferior knee. It is anteriorly connected with the transverse colon and mesocolon, the mesentery, and the loops of small bowel; posteriorly, with the abdominal wall and the medial margin of the right kidney; laterally, on the right, with the visceral face of the right hepatic lobe; and medially, on the left side, with the head of the pancreas.
The transverse part (third part) of the duodenum originates from the right duodenal flexure; it passes over the medial line and reaches the left flexure, where it starts ascending; it is connected, above, with the head of the pancreas; below, with the root of the mesentery; anteriorly, with the loops of the small intestine mesentery; and, posteriorly, with the abdominal wall.
The ascending part (fourth part) is on the left side of the median line; it originates from the left duodenal flexure and goes upward; it terminates at the level of the second lumbar vertebra where it continues into the jejunum through a sudden curve, the duodenojejunal flexure (where the suspensory musculotendinous ligament of the duodenum, or ligament of Treitz, is attached). It is anteriorly connected to the colon, the transverse mesocolon, and the first loops of the jejunum; posteriorly, with the body of the pancreas; and medially, with the head of the pancreas.
The vascularization of the duodenum is provided by the celiac trunk, which, through the superior pancreaticoduodenal artery (branch of the gastroduodenal artery), supplies the first and second parts of the duodenum, up to the major papilla; the inferior pancreaticoduodenal artery, originating from the superior mesenteric artery, supplies the third and fourth part. All the duodenal veins, either directly or indirectly, flow into the portal vein.
The lymph nodes of the duodenum originate from the submucosa, which also receives the lymph vessels coming from the tunica mucosa and muscularis; the lymph collectors heading toward the gastric lymph nodes depart from here.
The duodenal nerves originate from the orthosympathetic trunk and the parasympathetic innervation forms the vagus nerve through the celiac plexus.
8.1.3.2 Small Bowel (Jejunum and Ileum)
The small bowel is the longest part of the alimentary tract: it begins at the duodenojejunal flexure and enters the large intestine through the ileocecal valve. Its average length is 6–7 m and, considering the relatively small space in which it is contained, it forms several loops and circular convolutions, apparently located in a casual way, but actually organized in four groups: the first one in the left upper quadrant, the second in mesogastric region, the third one in the left iliac fossa, and the fourth in median position, between the right and left psoas muscles.
The small intestine mesentery is divided into two parts: the proximal 2/5 coincide with the jejunum (the name derives from the fact that in dead bodies, it is usually empty), and the distal 3/5, with the ileum (from the Greek word eileόs, for twisted). The two parts are not clearly separated: the jejunum is characterized by a slightly wider lumen and thicker, more vascular walls, with tall closely spaced circular folds (referred to as valvulae conniventes), few lymphoid nodules (Peyer patches) in submucosa, and a bigger amount of villi and glands.
The jejunoileal loops are anterolaterally covered, for a variable extension, by the greater omentum; posteriorly, there are next the retroperitoneal space and the organs contained therein (duodenum, uncinate process of the pancreas, kidneys, aorta, inferior vena cava, bodies of the last lumbar vertebrae); superiorly, to the transverse mesocolon and colon, separating the loops from the other viscera of the supramesocolic region (liver and spleen); laterally, they are adjacent to the cecum and the ascending colon, on the right, and the descending colon, on the left; and inferiorly, the loops of the small intestine enter the iliac fossa.
The wall of the small intestine is composed of four layers which are well visible through ultrasound examination: tunica serosa, extremely thin and formed by the peritoneum; tunica muscularis, with a longitudinal external layer and an internal circular one; tela submucosa, consisting of soft connective tissue; and the tunica mucosa, consisting of three typical structures, circular folds, villi, and intestinal glands which are well visible in macroscopic examinations. The circular folds (or valves of Kerkring) are permanent, semilunar valvular plicae of about 6–8 mm in the intestinal mucosa; they consist of two layers of mucosa with a central core of connective tissue between them, coming from the submucosa and contains vessels and nerves; they are located in the descending part of the duodenum and are less numerous in the last 60–80 cm, from the ileocecal valve. Their direct examination through endoscopy (video capsule endoscopy, double-balloon enteroscopy) or indirect examination through X-ray techniques (CT enterography/MRI enterography or small bowel enema) is essential for a correct study of the small intestine. The intestinal villi are fingerlike projections that protrude from the mucosa, each villus is approximately 1 mm long, and it is characterized by supportive tissue full of lymphatic and blood capillaries. They cover the whole mucosa of the small intestine. The circular folds, along with the villi, expand significantly the contact between the walls of the intestine and its content. After digestion, in fact, nutrients (such as sugar, proteins, fat acids, glycerol, and vitamins) are absorbed by the intestinal villi and transferred into the blood and lymph vessels. Some fat acids, namely, cholesterol and liposoluble vitamins, are absorbed through the lacteals and transferred, along with the lymph, to the thoracic duct, which flows into the left subclavian vein. Monosaccharides, amino acids, glycerol, mineral salts, hydrosoluble vitamins, and some fat acids are transferred to the portal vein, and then to the liver, by the capillaries. Physiologically, by extremely simplifying, we can say that the digestive process terminates in the jejunoileal loops, where the intestinal juices are produced (merged with bile and pancreatic juice) by the intestine walls, and most nutrient molecules are absorbed in this area. The undigested remains are pushed into the colon by peristalsis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


