Chapter 124 Overview: The kidney is the third most frequently injured abdominal viscus in children and accounts for 1.3% to 15% of injuries in children who suffer blunt abdominal trauma. Children are more susceptible to renal injury during blunt trauma compared with adults because of the relatively increased mobility of the pediatric kidney, less perinephric fat, and reduced protection by a more compliant chest wall. Preexisting renal abnormalities such as a horseshoe kidney (Fig. 124-1) or pelvic kidney, hydronephrosis, cystic renal disease, and tumors may increase the size or alter the location of the kidney leading to an increased susceptibility to injury.1 Figure 124-1 Laceration in horseshoe kidney. Most children with clinically significant renal injury present with hematuria; the risk of underlying renal injury is markedly higher in patients with gross hematuria (22%) compared with those with lesser amounts of urinary blood (8%). However, the presence of asymptomatic microscopic hematuria is a low-yield sign for the presence of underlying renal injury.2 Imaging: Computed tomography (CT) is the preferred modality for initial assessment of hemodynamically stable children with suspected renal injury because of its wide availability, rapid image acquisition, and accuracy. The use of intravenous contrast material is essential for the evaluation of the kidney, and scanning during the mixed venous phase of opacification is recommended. A delayed scan may be helpful for the detection of urinary extravasation. Noncontrast scans are not generally helpful, and they unnecessarily increase radiation dose to the patient. Unstable patients who require immediate evaluation may be examined with ultrasonography at the bedside prior to complete resuscitation or surgery. Routine follow-up imaging can be performed with grey-scale and color Doppler ultrasonography in most patients, and CT can be reserved for selected patients with other associated injury or ambiguous findings on serial ultrasonography.3 The most common type of renal injury is parenchymal contusion, which manifests on CT as a focal or diffuse region of absent or delayed contrast enhancement (Fig. 124-2). The contusion is characterized by microscopic areas of hemorrhage and surrounding edema. The involved kidney may also appear larger on CT as a result of the associated edema. Figure 124-2 Renal contusion. Renal collecting system injury results in urinary extravasation of intravenous contrast medium (Fig. 124-3). Urine leakage that remains encapsulated in the perirenal space is termed a urinoma. Occasionally, hemorrhage or urinary extravasation may extend into the pelvis owing to direct communication between the perirenal space in the abdomen and the prevesical extraperitoneal space in the pelvis.1 Figure 124-3 Grade IV renal laceration. The American Association for the Surgery of Trauma has developed an injury scale to categorize the increasing severity of renal injury (Table 124-1). Grade I to grade III injuries are considered low grade, and account for between 69% to 99% of all renal injuries. Table 124-1 Treatment: The great majority of renal injuries (69%–99%) are treated nonsurgically with great success. Even in high-grade injuries, no surgical intervention is necessary in 60% to 70%. Early ureteral stent placement may be considered in patients with high-grade injuries who do not demonstrate contrast material in the ipsilateral ureter.4 Overview: Blunt injuries to the bladder typically result from a blow to the lower abdomen when the bladder is distended or when the pelvis is fractured. Fortunately, the incidence of lower urinary tract injury in children is quite low, estimated at 0.2% of pediatric trauma admissions. Although approximately 50% of children with bladder tears have a pelvic fracture, only 0.5% to 3.7% of children with pelvic fractures have associated bladder injuries.5 High-yield indications for CT cystography include gross hematuria, pelvic fracture, and high-risk mechanisms of injury such as motor vehicle crashes and the presence of a seatbelt ecchymosis. Bladder injuries may be classified as intraperitoneal rupture, extraperitoneal rupture, and combined lesions. Imaging: Standard abdominal trauma CT scanning protocols may miss important bladder injuries because of incomplete bladder distention. CT cystography is the preferred technique for the detection of bladder tears with a reported sensitivity and specificity of 95% and 100% respectively.6
Genitourinary Trauma
Renal Injury
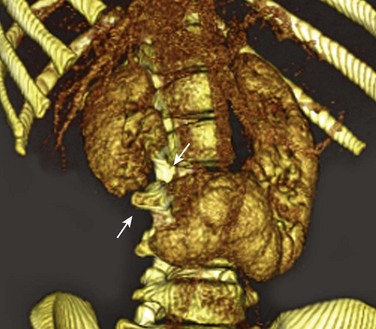
Oblique three-dimensional volume reconstruction of contrast-enhanced computed tomography shows complete transection (arrows) of a horseshoe kidney.

A contrast-enhanced coronal computed tomography image shows markedly diminished enhancement of the upper pole of the left kidney with preservation of renal contour.
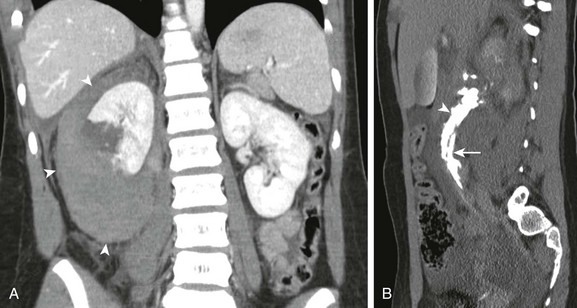
A, Coronal contrast-enhanced computed tomography shows complete transection of right kidney and large perinephric hematoma (arrowheads). B, A delayed sagittal-reformatted computed tomography scan shows extravasation of contrast-containing urine (arrowhead) along the right ureter (arrow).
Injury Grade
Renal Injury
I
Renal contusion, small, nonexpanding subcapsular hematoma
II
Superficial renal laceration not involving collecting system or deep medulla, nonexpanding perinephric hematoma
III
Deep renal laceration without involvement of renal collecting system, nonexpanding perinephric hematoma
IV
Laceration of renal collecting system, involvement of vascular pedicle
V
Shattered kidney, multiple lacerations, renal fragmentation
Bladder Injury
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree







