Fig. 3.1
Anatomy of nasal cavities and maxillary sinuses, caudal view. Medial pterygoid muscle (1), lateral pterygoid muscle (2), masseter (3), inferior turbinate (4), inferior meatus (5), nasal septum (6). Nasopharynx (N), maxillary sinus (asterisk)
Each nasal cavity is delimited below by the palatine bone, above by the cribriform plate of the ethmoid bone, and laterally by a wall in which we can easily recognize the lower and the middle turbinates (or nasal concha); at the cranial level, we find the superior turbinate and, less frequently, the supreme turbinate. The inferior turbinate is a separate bony structure, embryologically differentiated from the others that are, instead, related to the ethmoid.
The spaces between the turbinates and the side walls of the nose are defined meatus; in the anterior segment of the lower one, we find the end of the nasolacrimal duct.
3.1.1.2 Paranasal Sinuses
The paranasal sinuses are air-filled cavities more or less voluminous, interrelated with each other and, located in the facial skeleton, in the bones surrounding the nasal fossae (Fig. 3.2). Proceeding from the top to the bottom, we distinguish the frontal, the ethmoid, the sphenoid, and the maxillary sinuses.
Fig. 3.2
Anatomy of the facial skeleton, coronal section. Tongue (T), maxillary sinus (star)
The frontal sinus, placed between the two plates of the frontal bone, is divided by the septum into two cavities, often asymmetrical: it is connected with the nasal cavity through the frontonasal middle meatus recess. Changes in shape and size are significant: the sinus can be reduced to a cell located on the superomedial corner of the orbit, or it can be expanded along the supraorbital arch, up to the lesser sphenoid wings.
The ethmoid sinus is different from the other sinuses because it is composed by a set of small pneumatized cells, separated into anterior, middle, and posterior groups, forming an actual labyrinth, which is often subject to inflammatory processes. The ethmoid cells communicate with the nasal choanae through a series of microscopic orifices; in particular the anterior group opens in the hiatus semilunaris, the middle group in a bulge of the ethmoid, called ethmoid bulla (it is always in the middle meatus), and the posterior ones, in the superior meatus.
The sphenoid sinus is a pneumatized cavity located in the body of the sphenoid bone; this is also even and symmetrical and divided by an osseous septum variably centered with respect to the plane of symmetry. The opening of the sphenoid sinus is located in the terminal portion of the vault of the nasal fossa.
Among the paranasal cavities, the most pneumatized are the maxillary sinuses, represented by two cavities, approximately triangular, with the apex facing toward the zygomatic bone; they communicate with the middle meatus through an orifice called the hiatus semilunaris.
The ostiomeatal complex, frequently subject to obstructive diseases, is the anatomical and functional unit (that consists of middle turbinate and meatus, hiatus semilunaris, frontonasal recess, and ethmoid cells orifices) through which normal ventilation phenomena occur, along with the mucociliary clearance of the frontal, maxillary, and anterior ethmoid sinus cavity.
3.1.2 Normal Imaging Anatomy
3.1.2.1 Conventional Radiology
For many years the conventional radiology (CR) examination has been the only instrument available to radiologists and otolaryngologists for the examination of the paranasal sinuses, documenting the anatomy of the frontal, maxillary, and sphenoid sinuses, but not the changes in the mucosa and thinner bone structures, such as the ethmoid cells.
The most commonly used radiographic projections are the lateral projections and the Caldwell’s and Waters’ views. The first one is irreplaceable and, therefore, included in every protocol study of the skull. In case of difficult patients (uncooperative or traumatized), it can be performed in supine position, or in sitting position, using a craniostat. The right projection will provide the perfect overlap of the symmetrical structures (such as the greater wings of the sphenoid bone or the ascending mandibular branches), the adequate representation of the internal and external plates of the cranial vault, as well as the sella turcica. It provides a good display of almost all the paranasal sinuses and also of skull and sella turcica (Fig. 3.3).

Fig. 3.3
Paranasal cavities X-ray, lateral view. Sella turcica (arrowhead), frontal sinus (1), maxillary sinus (2), sphenoid sinus (3)
The Caldwell’s view is performed with the patient in prone position, his head leaning against the frontal bone and nose and the central oblique X-ray beam, on the sagittal plane, craniocaudally tilted of 15/25°, in posterior-anterior direction. The symmetrical representation of all the even bones of the skull, the orbits and the petrous bones, the latter included in the lower half of the orbit, is the reference accuracy criteria. Such a projection allows the proper evaluation of the frontal sinuses, the ethmoid cells, the nasal cavities, and the cranial vault (Fig. 3.4).

Fig. 3.4
Paranasal cavities X-ray, Caldwell’s projection. Frontal sinus (1), maxillary sinus (2), inferior turbinate (3), nasal septum (4), ethmoid cells (5), petrous bones (6)
The Waters’ view has a difficult and controversial codification, and it is not easy to perform: the orbitomeatal line must be, in fact, precisely at an angle of 37° with the X-ray plate and the head rest on the single, unstable chin support with open mouth; a symmetrical view of all the structures of the skull is required; the sphenoid sinus must project into the buccal opening, below the upper teeth; the lower border of the mandible and the occipital margin should be displayed on a single line. The Waters’ view clearly shows the paranasal sinuses quite well (particularly the frontal and maxillary sinuses), the nasal cavities, the zygomatic arches, and the orbit structures (Fig. 3.5).

Fig. 3.5
Paranasal cavities X-ray, Waters’ projection. Frontal sinus (1), maxillary sinus (2), sphenoid sinus (3), nasal fossa (4), orbit (5)
Furthermore, a fourth type of projection that can be performed is the Hirtz view (submental vertex view), less common than the previous projections.
3.1.3 Computed Tomography
Computed tomography (CT) has relegated conventional radiology to a marginal role in the study of the paranasal cavities; this technique allows a much finer description of the complex anatomy of such a region.
The exam is almost always performed without intravenous contrast agent, with the scans extended from the frontal sinus to the hard palate, with a thickness of ≤1 mm.
The axial scans allow a good evaluation of all the bony structures of the paranasal sinuses and, above all, of the ostiomeatal unit; they are particularly suitable for the evaluation of the sphenoethmoidal and frontal recesses and of the anterior, the middle, and the posterior ethmoidal cells (Fig. 3.6). On the axial plane, it is also possible to see the adjacent structures, such as the epipharynx in which you can clearly recognize the torus tubarius and the lateral recess, and easily highlight possible asymmetries (Figs. 3.7).
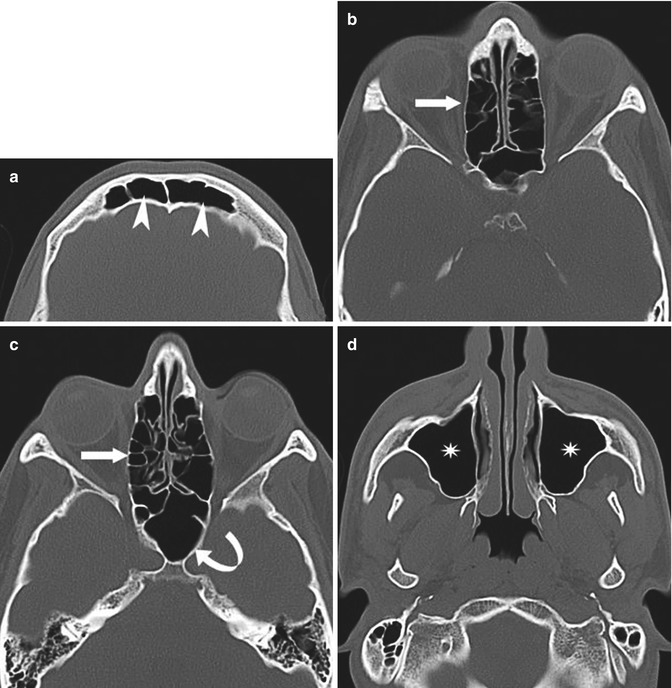
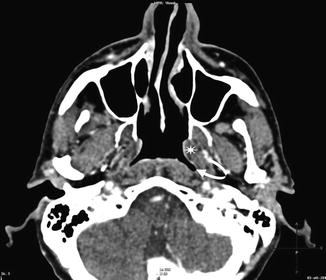
Fig. 3.6
Paranasal cavities CT, axial scan, with high-spatial-frequency (bone) reconstruction algorithm. (a) Frontal sinuses (arrowhead). (b) Ethmoid cells (arrow). (c) Ethmoid cells (arrow) and sphenoid sinus (curved arrow). (d) Maxillary sinus (asterisks)
Fig. 3.7
Paranasal cavities CT scan, axial scan with a window setting for the soft part. Lateral epipharyngeal recess (curved arrow), torus tubarius (asterisk)
The coronal reconstructions of the facial skeleton are very important because they allow to easily recognize, and precisely analyze, the ostiomeatal complex (Fig. 3.8). CT allows the precise assessment of the bone anatomic variants of the paranasal sinuses. This information is a matter of great importance, because it may change the surgical planning. As an example, the concha bullosa (consisting of a pneumatization of the middle turbinate) and the Onodi cell (a posterior ethmoid air cell that lies superior to the sphenoid sinus and it is in close proximity to at least one optic nerve or internal carotid artery) can be mentioned (Fig. 3.9).
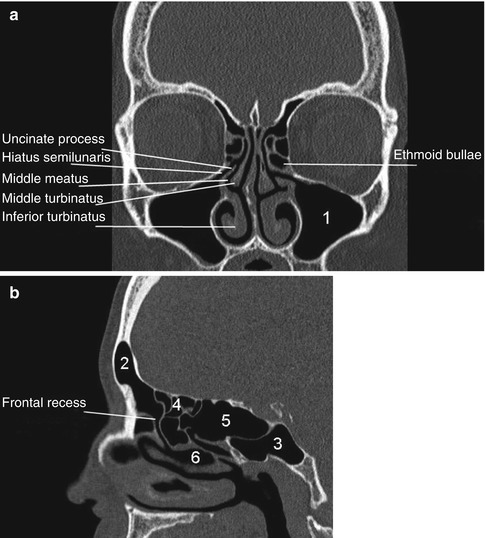
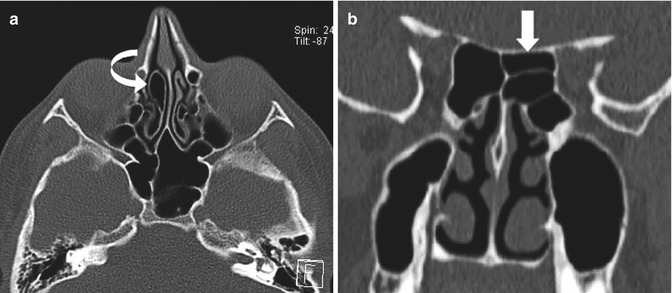
Fig. 3.8
Paranasal cavities CT scan, coronal (a) and sagittal (b) scan, with high-spatial-frequency (bone) reconstruction algorithm. Maxillary sinus (1), frontal sinus (2), sphenoid sinus (3), ethmoid cells (4), Onodi cell (5), middle meatus (6)
Fig. 3.9
Paranasal cavities CT scan, axial (a) and coronal imaging (b), with high-spatial-frequency (bone) reconstruction algorithm. (a) Concha bullosa (curved arrow). (b) Onodi cell (arrow)
3.1.3.1 Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) of the head gives very specific information, but it cannot provide precise information about the bone structures, as the CT examination does; therefore, it has to be performed accordingly (especially for the facial bones, mostly composed of cortical material). The essential advantage of the MRI examination is the peculiar capacity to identify the mucosal tissue (Fig. 3.10).
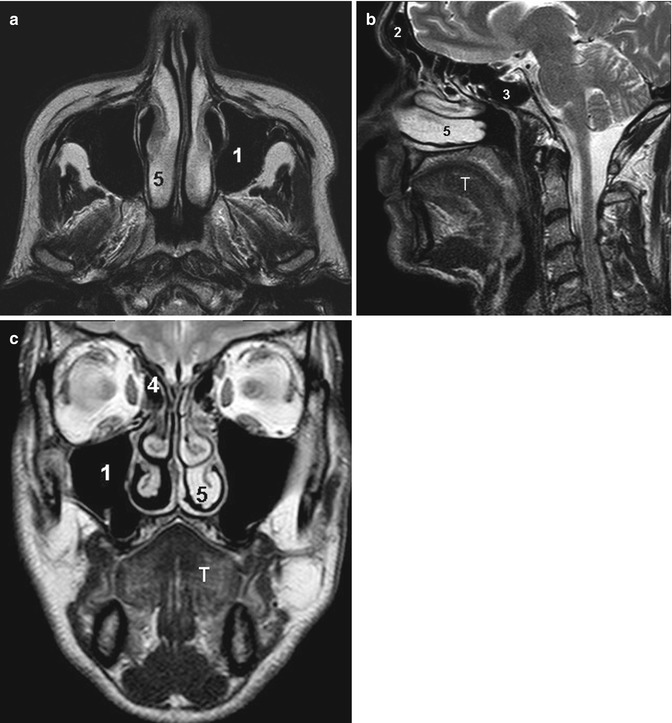
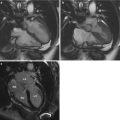
Fig. 3.10
Nasal cavities MRI T2-weighted axial (a), sagittal (b), and coronal (c). Tongue (T), maxillary sinus (1), frontal sinus (2), sphenoid sinus (3), ethmoid cells (4), inferior turbinate (5)
3.2 Neck
3.2.1 Normal Anatomy
In the neck we can distinguish the oral cavity, the pharynx (divided in rhinopharynx, oropharynx, and hypopharynx), and the larynx; we can also find lymph nodes and glandular structures, the thyroid and salivary glands.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


