Secondary: Due to increased iron intake, transfusions, etc.
• Hemosiderosis
Increased iron deposition without organ damage
IMAGING
• Liver that is hyperdense on NECT and markedly hypointense on T2WI or in-phase GRE MR
• Primary (hereditary) hemochromatosis
Affects parenchymal cells of liver, pancreas, and heart
• Secondary hemochromatosis
Affects RES: Liver, spleen, nodes
TOP DIFFERENTIAL DIAGNOSES
• Amiodarone therapy
• Glycogen storage disease
PATHOLOGY
• Primary (hereditary) hemochromatosis
Relatively common and underdiagnosed cause of liver disease
Affects 1 in 220 of some European groups
Clinical: Cirrhosis and “bronze diabetes”
Progressive injury of heart, liver, and pancreas
Increased risk of hepatocellular carcinoma
DIAGNOSTIC CHECKLIST
• T2WI: Marked signal loss of liver in primary type and marked signal loss of both liver and spleen in secondary type of hemochromatosis
• Due to phlebotomy or chelation, liver may appear as normal attenuation on CT
(Left) In this case of primary (hereditary) hemochromatosis, coarse and refractile iron granules are readily discernible within the hepatocytes and bile duct epithelium. (Courtesy M. Yeh, MD, PhD.)
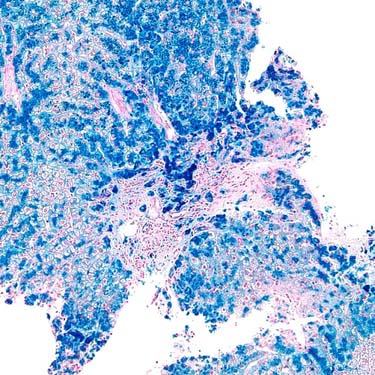
(Right) The iron deposition is confirmed by a Perl iron stain. (Courtesy M. Yeh, MD, PhD.)
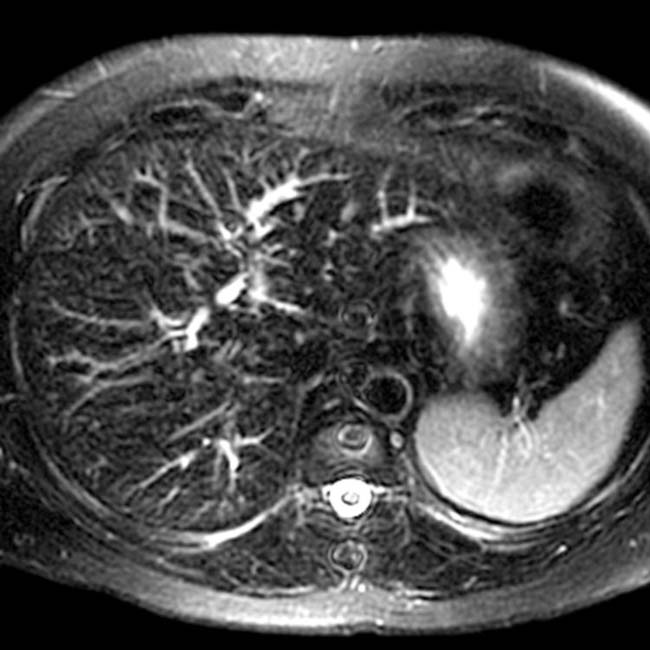
(Left) Axial T2WI MR shows marked hypointensity throughout the liver in this patient with primary (hereditary) hemochromatosis. Note the normal intensity of the spleen by comparison.
(Right) In this patient with secondary hemochromatosis due to blood transfusions, axial NECT shows marked diffuse increased density in the liver. The spleen is surgically absent.
TERMINOLOGY
Definitions
• Iron overload disorder in which there is structural and functional impairment of involved organs
• Hemosiderosis
Increased iron deposition without organ damage
Usually seen with body iron stores of 10-20 g
IMAGING
General Features
• Best diagnostic clue
Liver that is hyperdense on NECT and markedly hypointense on T2WI or in-phase GRE MR
• Location
Primary (hereditary) hemochromatosis
– Parenchymal cells of liver, pancreas, and heart
Secondary hemochromatosis
– Initially affects reticuloendothelial system (RES)
Liver, spleen, and lymph nodes, bone marrow
– After saturation of RES, then parenchymal cells of liver, pancreas, myocardium, kidneys, and endocrine glands
• Key concepts
Hemochromatosis: Classified into 2 types
– Primary (hereditary)
Autosomal recessive disorder causing increased absorption of iron from gut
Affects parenchyma of liver, heart, pancreas
– Secondary
Due to multiple blood transfusions, increased iron intake, etc.
Affects reticuloendothelial system (RES) (liver, spleen, nodes, marrow)
– Total body iron may be 50-60 g
Normal body iron storage: 2-6 g of iron
– 80% of iron in functional form: Hemoglobin, myoglobin, and iron-containing enzymes
– 20% of iron in storage form: Hemosiderin or ferritin
– Liver contains up to 1/3 of body’s total iron store
CT Findings
• NECT
Homogeneously increased liver density
– Up to 75-135 HU (normal 45-65 HU)
Conspicuous low-attenuated hepatic and portal veins
Dual energy CT (at 80 and 120 kVp) technique used to
– Establish diagnosis if attenuation is borderline
– Quantify amount of iron deposition in liver
– Follow efficacy of therapy
• CECT
Makes excess iron in liver or spleen less apparent
Late stage: features of cirrhosis ± portal hypertension
MR Findings
• T1WI
Decreased signal intensity in liver
• T2WI
Primary: Marked signal loss in liver ± pancreas, heart, etc.
Secondary: Marked signal loss in both liver and spleen
• T1WI GRE
Signal dropout from liver on in-phase
Opposite of what occurs in steatosis (which is signal dropout on opposed-phase GRE)
Ultrasonographic Findings
• Grayscale ultrasound
Has no role in diagnosis of hepatic iron overload
Only gold members can continue reading. Log In or Register to continue









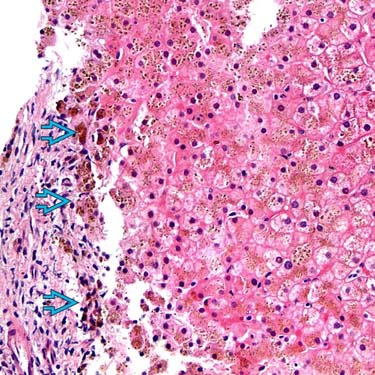
 are readily discernible within the hepatocytes and bile duct epithelium. (Courtesy M. Yeh, MD, PhD.)
are readily discernible within the hepatocytes and bile duct epithelium. (Courtesy M. Yeh, MD, PhD.)