Plantar plate tears are a significant cause of forefoot pain and functional disability, frequently underdiagnosed due to their nonspecific clinical presentation and overlap with other causes of metatarsalgia. As the primary static stabilizers of the lesser metatarsophalangeal joints, plantar plates are subject to degenerative and traumatic injuries, particularly in specific at-risk populations. Accurate diagnosis necessitates high-resolution imaging modalities, with ultrasound offering a cost-effective, dynamic option, and MR imaging, particularly 3D isotropic sequences, providing superior anatomic detail for precise assessment.
Key points
-
•
Plantar plate tears are a major cause of lesser metatarsophalangeal joint instability and forefoot pain.
-
•
Imaging is essential for diagnosis, with ultrasound offering dynamic evaluation and MR imaging providing superior imaging contrast and anatomic detail.
-
•
Early detection and accurate diagnosis can prevent long-term disability and deformity.
-
•
Emerging imaging technologies such as 3D MR imaging acquisition with multiplanar reconstructions and AI tools show promise for future advancements in diagnosis and treatment planning.
Abbreviations
| MTP | metatarsophalangeal |
| STIR | short tau inversion recovery |
| USG | ultrasound |
Introduction
The plantar plate is a critical fibrocartilaginous structure located at the plantar aspect of the metatarsophalangeal (MTP) joints. It functions as a key static stabilizer by resisting hyperextension forces and maintaining the alignment of the toes during ambulation. Structurally, the plantar plate is composed predominantly of type I collagen arranged in longitudinal fibers, akin to meniscal architecture, conferring tensile strength along the longitudinal axis and resistance to compressive loads.
Injuries to the plantar plate are one of the causes of metatarsalgia, acute or chronic pain at one or more MTP joints. The injured and dysfunctional plantar plate causes joint instability, altered biomechanics, and deformity. Despite their prevalence, plantar plate tears often remain underdiagnosed due to their insidious onset and overlapping clinical presentation with other causes of metatarsalgia, such as Morton’s neuroma or intermetatarsal bursitis.
Accurate diagnosis is paramount to prevent progression to fixed deformities, such as crossover toe or hammer toe, which may require more complex surgical correction. Imaging modalities, particularly ultrasound (USG) and MR imaging, play a crucial role in diagnosing plantar plate tears. This article aims to provide a comprehensive synthesis of the clinical presentation, imaging findings, and comparative diagnostic performance of USG and MR imaging, with a special focus on emerging 3D isotropic MR imaging techniques.
Epidemiology and health care system impact
Prevalence and Risk Factors
Plantar plate tears primarily affect middle-aged women and young athletes, with degenerative changes being the leading cause in the former and traumatic injuries more prevalent in the latter. The second MTP joint is the most frequently involved site, attributed to the higher biomechanical load borne by the second ray during the gait cycle. In a degenerative case, chronic repetitive microtrauma leads to fibrocartilaginous degeneration, reduced tensile strength, and eventual partial or complete tearing. Traumatic mechanisms often involve acute hyperextension injuries common in athletes, can exceed the tensile limits of the plantar plate, and result in rupture.
Several risk factors contribute to the development of plantar plate tears. Pes cavus deformity, metatarsus adductus, and forefoot varus in isolation or combined can increase forefoot load and predispose the plantar plate to injury. A long second metatarsal enhances mechanical leverage at the MTP joint, increasing the likelihood of plantar plate stress and subsequent tearing. Footwear factors, particularly the use of high-heeled shoes or those with a narrow toe box, elevate forefoot pressure and contribute to plantar plate degeneration and tearing. Systemic conditions, such as rheumatoid arthritis, may also predispose individuals to plantar plate tears through mechanisms involving chronic synovitis and joint instability.
Reported prevalence in surgical series evaluating forefoot pain suggests that plantar plate tears account for a significant proportion of lesser toe deformities and MTP joint instability cases.
The economic burden associated with plantar plate tears is multifactorial. Although direct costs with diagnosis, conservative treatment or surgical interventions should be taken into consideration, it is the indirect costs that cause the most substantial economic impact with loss of productivity, chronic disability, and the impact on quality of life, which can be prevented or attenuated with early diagnosis and appropriate treatment. Though exact figures for the economic impact of plantar plate tears in the United States are not available at the time of this writing, it is likely a figure in the tens of millions if not more after considering direct and indirect costs, particularly in athletes.
Complications
Long-Term Sequelae
Without appropriate diagnosis and management, plantar plate tears may progress to several debilitating complications. Chronic MTP joint instability often develops as the stabilizing function of the plantar plate deteriorates. Patients may subsequently develop crossover toe deformity, characterized by dorsomedial subluxation of the affected toe, and hammer toe deformity, both of which compromise foot biomechanics and aesthetics. Painful callus formation frequently occurs because of abnormal pressure distribution across the plantar surface.
Additionally, gait abnormalities and compensatory mechanics may emerge, further exacerbating functional impairment. Secondary metatarsalgia can develop, affecting adjacent metatarsals due to altered load transmission. These sequelae significantly impair ambulation and reduce quality of life, underlining the necessity for early diagnosis and intervention.
Injuries most frequently occur at the distal insertion on the proximal phalanx and typically involve the lateral aspect. Progressive tearing can compromise the collateral ligaments and adjacent stabilizing structures, resulting in MTP joint subluxation, deformity, and functional impairment.
Clinical presentation
Patients with plantar plate injuries often report localized forefoot pain, particularly under the second or third MTP joints. , Many describe a sensation akin to “walking on a marble,” which reflects the underlying instability and subluxation associated with the injury. , Progressive deformity is another hallmark, with patients initially noticing a widening of the interdigital space, followed by visible dorsal subluxation and eventual crossover toe deformity. Symptoms are typically exacerbated by weight-bearing activities, especially during the push-off phase of gait. Notably, patients with plantar plate injuries usually do not experience neuropathic symptoms, a distinguishing feature that helps differentiate this condition from Morton’s neuroma, where burning or tingling sensations are common.
Differential Diagnosis
Several conditions can mimic the clinical presentation of plantar plate. Morton’s neuroma presents as a compressible mass-like lesion between the metatarsal heads, causing burning pain and paresthesia radiating distally; ultrasound (USG) may reveal a hypoechoic mass, while MR imaging typically shows an intermetatarsal space lesion (a neuromal–bursal complex) with low T1 and high T2 signal intensity. Intermetatarsal bursitis, characterized by inflammation of the bursa between 2 metatarsal heads, can similarly cause forefoot pain but generally lacks the structural deformities associated with plantar plate pathology.
Freiberg’s infraction, osteonecrosis of the metatarsal head (most commonly second) results in joint pain and stiffness, with radiographs or MR imaging demonstrating articular surface collapse and fragmentation. Stress fractures involving the metatarsal shaft or neck present with localized tenderness and can be confirmed using MR imaging or bone scintigraphy. Plantar vein thrombosis, although rare, is another potential cause of plantar pain and swelling; diagnosis can be aided by USG with Doppler evaluation, which may reveal thrombosed plantar veins. Finally, sesamoiditis, an inflammation of the sesamoid bones beneath the first MTP joint, typically results in medial plantar pain localized to the area beneath the first metatarsal head.
Careful clinical assessment combined with targeted imaging is essential for accurate diagnosis.
Imaging modalities: ultrasound
Technique
USG offers several advantages for the evaluation of plantar plate injuries. It allows real-time dynamic assessment and is both cost-effective and widely available. Importantly, extremities are not common sites of fat accumulation, making forefoot USG diagnostic performance in obese patients less affected than other body parts, such as the hips or shoulders.
USG evaluation of the plantar plate is typically performed using a high-frequency (8–18 MHz) linear transducer. Use of USG is operator-dependent and demonstrates reduced sensitivity for detecting partial-thickness tears compared to MR imaging. The examination is best conducted with the patient in the supine position and the foot dorsiflexed to optimize exposure of the MTP joint. Dynamic maneuvers are particularly useful, enhancing the detection of plantar plate insufficiency by visualizing abnormal motion of the proximal phalanx relative to the metatarsal head.
Findings
On ultrasonography, the normal plantar plate appears as a hyperechogenic structure situated between the cartilage and the flexor tendon ( Fig. 1 ). USG imaging can reveal both direct and indirect signs of plantar plate pathology. Direct signs include a hypoechoic or anechoic defect within the plantar plate and thinning or discontinuity of its fibrillar architecture ( Fig. 2 ). Indirect signs comprise pericapsular fibrosis, often presenting a pseudoneuroma appearance, flexor tendon sheath effusion, and evidence of MTP joint subluxation during dynamic examination.
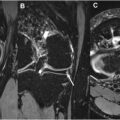
Ultrasonographic appearance of a normal plantar plate. ( A – D ): Second metatarsophalangeal (MTP) joint sagittal view in neutral position ( A ) and extension ( B ). Parasagittal views along the lateral ( C ) and medial aspects of the joint. Second metatarsal head ( asterisk ) and cartilage ( short arrow ). Hyperechogenic plantar plate lying between the cartilage and flexor tendon ( curved arrow ). Note the normal insertion of the plantar plate at the proximal phalanx base on sagittal and parasagittal images ( long arrow ). ( E ) Transverse view of the second MTP joint depicting normal features of the plantar plate medial ( short arrow ) and lateral ( long arrow ) segments, with overlying normal flexor tendons ( curved arrow ).
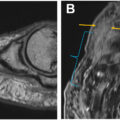
A-C: Plantar plate tear. A–C: Second metatarsophalangeal (MTP) joint median sagittal view ( A ), medial ( B ), and lateral ( C ) paramedian sagittal views demonstrating the normal appearance of the phalangeal insertion centrally ( A ) and medially ( B ), but heterogenous lateral insertion with partial discontinuity. ( D – E ): Transverse views. Normal hyperecogenic lateral plantar plate segment at the level of the metatarsal head ( curved arrow on D) but partial discontinuity more distally ( curved arrow on E) with surrounding edema ( short arrow ).
Imaging Protocol
For optimal evaluation, a high-frequency linear probe (8–20 MHz) should be employed. The patient is positioned supine with the foot dorsiflexed; this positioning can be modified as needed to facilitate dynamic examination. The technique involves obtaining longitudinal and transverse scans of the plantar aspect of the MTP joints. Dynamic stress maneuvers, such as dorsiflexion and plantarflexion of the toes, are useful for assessing plantar plate motion and stability. Additionally, applying Doppler settings can help evaluate associated bursitis or vascular involvement.
Certain technical considerations are crucial for image quality. Optimal gel application without compression is necessary to minimize artifacts, and bilateral comparison may be valuable in detecting subtle or equivocal cases.
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 High-Resolution Imaging of Knee Meniscus Anatomy and Tears
High-Resolution Imaging of Knee Meniscus Anatomy and Tears
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


