MR imaging plays a critical role in evaluating elbow ligament pathologies and associated instability and impingement syndromes. The article details standard and advanced elbow MR imaging techniques and highlights the normal anatomy of the medial and lateral elbow ligament complexes. High-field strength magnets, dedicated surface coils, optimized patient positioning, three-dimensional imaging, and deep learning reconstructions enhance visualization of ligament structure and integrity. These measures facilitate assessment of conditions such as valgus extension overload, posteromedial and radiocapitellar impingement, and posterolateral rotatory instability syndrome. Recognition of both primary ligament injury and secondary joint changes enables precise diagnosis and guides targeted management.
Key points
-
•
Elbow injuries are common in both athletic and non-athletic populations.
-
•
Advanced MR imaging techniques may improve the detection and characterization of elbow pathologies.
-
•
Detailed anatomic knowledge and optimized imaging protocols are essential for the accurate diagnosis of elbow ligament injuries and impingement syndromes.
Abbreviations
| CT | computed tomography |
| LUCL | lateral ulnar collateral ligament |
| PLRI | posterolateral rotatory instability |
| RCL | radial collateral ligament |
| SNR | signal-to-noise ratio |
| UCL | ulnar collateral ligament |
Introduction
Elbow pain is a common presenting symptom in those seeking medical care. Beyond tendon pathology and arthritis, ligament injuries are frequent sequelae of repetitive stress or overuse and acute injuries. Several impingement and instability syndromes are associated with elbow ligament pathology and have characteristic injury mechanisms and imaging findings. MR imaging plays a critical role in evaluating ligamentous integrity and associated nonligamentous pathology in patients with these syndromes. This article details standard-of-care MR imaging techniques for the elbow along with select advanced techniques. We discuss ligamentous anatomy, pathology, and clinical sequelae of said pathology on the medial–ulnar side of the elbow followed by the lateral–radial side. By understanding the imaging appearance of both ligament injuries and their associated clinical sequelae, radiologists can deliver more useful interpretations that guide diagnosis, inform treatment strategies, and improve patient outcomes.
Imaging technique
Initial imaging for elbow pain is most frequently accomplished with radiography, which provides optimal spatial resolution for the assessment for osseous injury and may serve as a screening modality before cross-sectional imaging. MR imaging provides superior contrast resolution for soft tissue evaluation compared to computed tomography (CT). While MR imaging lacks the dynamic capabilities of ultrasound, it offers greater sensitivity for a wider range of pathologies, is less operator-dependent, and is more widely available given the dearth of dedicated musculoskeletal sonographers.
Elbow MR imaging should be performed at field strengths of 1.5 to 3.0 T, with 3.0 T preferred given its superior signal-to-noise ratio (SNR). Greater field strengths like 7.0 T have shown promise in the research setting but are not routinely used in clinical practice, limited largely by the availability of appropriate coils. Regardless of field strength, surface coils are necessary to achieve the requisite SNR for diagnostic imaging. Flexible phased-array coils are frequently used for elbow imaging as they can be wrapped around the elbow, allowing for close proximity to the anatomy of interest and adaptability to various body habitus. An alternative is the use of a rigid knee coil, which has a higher number of channels than many flexible coils, allowing for higher SNR. The rigid knee coil also has symmetric coil geometry, permitting the use of higher acceleration factors, and has radiofrequency transmit capability, reducing aliasing artifacts.
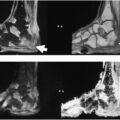
The two main choices for patient positioning are supine with the arm by the side and prone with the arm overhead (the superman position ) ( Fig. 1 A–C ). The supine position with the arm by the side affords the greatest comfort to the patient but sacrifices image quality because the elbow is off-center within the magnet; this position also introduces aliasing artifacts from excitation of anatomy adjacent to the arm. The prone position with the arm overhead is preferred, as this position places the elbow nearer to the isocenter of the magnet, maximizing field homogeneity and reducing aliasing artifacts. This position, however, may be less comfortable for patients, resulting in increased motion artifacts. Technologists can help patients tolerate positioning using cushions and support.
Elbow MR imaging patient positioning options. ( A ) Prone superman position with the arm above the head and the elbow centered in a rigid knee coil. ( B ) Prone superman position with the arm above the head and the elbow in a flexible surface coil. ( C ) Supine position with the arm by the side and the elbow in a flexible surface coil.
Reprinted with permission, Cleveland Clinic Foundation ©2025. All Rights Reserved.
Specialized positioning can be helpful in selected patients. For example, the flexed elbow valgus external rotation position places a valgus stress on the ulnotrochlear joint and allows for long-axis imaging of the ulnar collateral ligament (UCL) ( Figs. 2 A, B and 3 ).
( A ) Flexed elbow valgus external rotation (FEVER) position with elbow in 90° of flexion and shoulder in external rotation with weight on hand to apply valgus load. ( B ) FEVER position with flexible surface coil overlying elbow.
Flexed elbow valgus external rotation view demonstrating the ulnar collateral ligament in the long axis. There is minimally increased fluid signal at the humeral attachment ( arrow ) in this asymptomatic 24 year old major league baseball player.
The American College of Radiology Practice Parameter document for elbow MR imaging outlines technical considerations for protocol optimization. The routine protocol used at our institution is detailed in Table 1 . Deep learning MR imaging reconstruction techniques recently introduced by most major MR scanner manufacturers can help reduce image noise, increase spatial resolution (allowing for super resolution), and reduce acquisition times ( Fig. 4 ).
Table 1
Elbow MR imaging protocol
| Sequence | Field of View (mm) | Slice Thickness (mm) | Slice Gap (mm) | Repetition Time (ms) | Echo Time (ms) | Resolution |
|---|---|---|---|---|---|---|
| Axial T2 | 120 | 3 | 0.3 | 2000–5000 | 30 | 320 @ 80% |
| Axial T2 fat-saturated | 120 | 3 | 0.3 | 2000–5000 | 50–60 | 256 @ 100% |
| Coronal T2 fat-saturated | 120 | 3 | 0.3 | 2000–5000 | 10–15 | 256 @ 100% |
| Coronal T1 | 120 | 3 | 0.3 | 400–800 | 50–60 | 320 @ 80% |
| Sagittal T2 fat-saturated | 120 | 3 | 0.3 | 2000–5000 | 50–60 | 256 @ 100% |
Coronal inversion-weighted T2 fat-saturated images of 2 young adults of similar age, obtained on the same day on 1.5 T scanners. The left image, reconstructed with deep learning techniques, demonstrates decreased noise and improved spatial resolution compared to the right image without deep learning.
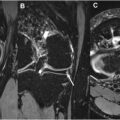
Supplementary sequences are sometimes obtained depending on the clinical scenario, including 3D sequences. 3D sequences with isotropic or near-isotropic voxels allow for acquisition of submillimeter slices, enabling custom reformatting in nonorthogonal planes at the time of image interpretation and enhancing elbow ligament assessment ( Fig. 5 A, B ).
( A ) Reformatted 3D MR imaging to optimize ulnar collateral ligament (UCL) visualization in 3 planes ( arrows ). ( B ) Enlarged reformatted long-axis image of the UCL ( arrows ).
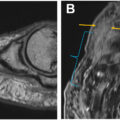
Intravenous contrast is not routinely indicated in MR imaging of the elbow. Intra-articular contrast (ie, MR arthrography) can be used but is not routinely performed. It may be useful in cases of posterolateral rotatory instability, suspected osteochondral injuries, or intra-articular bodies. MR arthrography may also increase sensitivity for partial-thickness tears of the mid-distal UCL ( Fig. 6 ), which can be meaningful in high-level athletes for whom these injuries can have serious implications. Sensitivity for proximal UCL tears, however, is lower with MR arthrography than with conventional MR imaging. MR arthrography may also be helpful in differentiating intermediate intrasubstance graft signal from graft tearing after UCL reconstruction, particularly articular-sided tears, but is not routinely used for this purpose. T2-weighted images should be included in MR arthrography protocols to enable visualization of tearing of the outer graft fibers, which might otherwise go undetected.
Coronal T1 fat-saturated image with intra-articular contrast demonstrates a small partial-thickness undersurface ulnar collateral ligament (UCL) tear at the sublime tubercle ( arrow , left ). Contrast extending over the sublime tubercle deep to the distal UCL fibers forms the characteristic T sign ( right ).
Anatomy, pathologies, and clinical significance
The ulnohumeral, radiocapitellar, and proximal radioulnar articulations, all contained within a common joint capsule, comprise the elbow joint. The ulnohumeral articulation along the medial aspect of the joint is a hinge joint formed by the trochlea of the humerus and the olecranon fossa of the ulna. It is the primary osseous stabilizer of the elbow. , The radiocapitellar joint along the lateral aspect of the elbow enables both hinging and rotation. The radial head rotates against the ulnar sigmoid notch at the proximal radioulnar joint.
Medial–Ulnar
Anatomy
The UCL is composed of anterior, posterior, and transverse bundles ( Figs. 7 and 8 ). The anterior bundle is the largest and most biomechanically important of the bundles, coursing from the anteroinferior aspect of the medial humeral epicondyle to the ulnar sublime tubercle and serving as the primary restraint against valgus stress. The anterior bundle is the component most seen on MR imaging on coronal images. The posterior bundle may also be seen on more posterior coronal images or on axial images deep to the ulnar nerve.
Sequential coronal T2 fat-saturated images of the normal ulnar collateral ligament (UCL) ( arrows ) from anterior ( left ) to posterior ( right ).
Illustration of the normal ulnar collateral ligament.
Reprinted with permission, Cleveland Clinic Foundation ©2025. All Rights Reserved.
On MR imaging, increased signal intensity along the deep aspect of the humeral attachment of the anterior bundle is a normal finding secondary to interdigitating fibrofatty tissue, which can result in a striated appearance of the proximal ligament. Distally, the ligament may attach beyond the articular surface of the ulna, complicating differentiation between normal and partial undersurface tears. The posterior bundle arises from the humerus more inferiorly and attaches to the trochlea, posterior to the sublime tubercle. The transverse bundle courses between the ulnar attachments of the anterior and posterior bundles and is of little biomechanical importance. An accessory UCL is present in nearly one-quarter of the population but is not typically evaluated on MR imaging.
The superficial aspect of the UCL is closely associated with the overlying flexor digitorum superficialis muscle, which is part of the flexor–pronator mass/muscle complex. These muscles provide dynamic stability against valgus stress, especially during the early acceleration phase of overhead throwing.
Pathologies and clinical significance
UCL injuries may occur after falls and elbow dislocations and are also seen secondary to excessive valgus stress, commonly in overhead throwing athletes, who endure extreme valgus forces about the elbow during the late cocking and acceleration phases. With repetition, these stresses may lead to adaptive ligament thickening and degeneration ( Fig. 9 ), sometimes presenting with increased intrasubstance fluid signal intensity and laxity. The imaging appearance of partial UCL tears may overlap with the appearance of chronic asymptomatic ligamentous remodeling or degeneration. Clinicians must therefore consider the imaging findings in combination with clinical history and physical examination findings in athletes with elbow pain. ,,,,
Sequential coronal T2 fat-saturated images of a 20 year old collegiate baseball pitcher show diffuse adaptive thickening of the ulnar collateral ligament ( arrows ), which is otherwise normal.
Injuries of the UCL may occur acutely, with or without a background of ligamentous degeneration. These injuries may occur in the ligament midsubstance or at or near the humeral and ulnar attachments; the literature reports conflicting predilections for tear location. ,,, A normal-appearing ligament with adjacent periligamentous edema is characteristic of an acute low-grade sprain. In overhead throwing athletes, this periligamentous edema is commonly seen adjacent to a ligament that is thickened from chronic biomechanical stress. Edema in the adjacent flexor–pronator mass due to concomitant muscle strain is not uncommon in the setting of UCL sprains, as these muscles provide dynamic restraint against valgus stress ( Fig. 10 ).
Coronal inversion-weighted fat-saturated image of a 16 year old baseball player shows a complete ulnar collateral ligament tear at the humeral attachment with distal retraction ( solid arrow ). There is surrounding edema and intermediate-grade strain of the flexor pronator mass ( open arrow ).
In addition to intrasubstance signal abnormality, partial tears may appear as fiber discontinuity not involving the full width of the ligament ( Figs. 11 A, B and 12 A, B ). Fiber tearing of less than and more than 50% of the ligament width is commonly categorized as low-grade and high-grade tearing, respectively. Discrete fiber discontinuity may be difficult to appreciate in the absence of fluid distention of the joint. The presence of periligamentous edema may support the diagnosis of a partial tear in these cases. Partial tears of the distal UCL deep fibers may have a characteristic appearance in which fluid signal extends between the sublime tubercle and the intact superficial ligament fibers, referred to as the T sign . It is essential to distinguish true fluid signal from the signal of the ulnar articular cartilage, as the ligament may insert up to 3 mm distal to the chondral margin; in such cases, normal chondral signal could be misinterpreted as a partial tear. Complete, full-thickness tears are a less challenging diagnosis, with fiber discontinuity extending across the full width of the ligament (see Figs. 10 and 13 A, B ).
( A ) Coronal T2 fat-saturated image of a 17 year old baseball pitcher demonstrates a high-grade ulnar collateral ligament tear at the sublime tubercle ( open arrow ). ( B ) More posteriorly, joint fluid extends distally under the ligament, forming the characteristic T sign ( arrowhead ). Periligamentous edema ( solid arrows ) suggests relatively acute injury.
( A ) Coronal proton density fat-saturated image of a 27 year old minor league baseball pitcher with history of remote ulnar collateral ligament (UCL) injury managed conservatively and new medial elbow pain. Intermediate signal and heterogeneity are seen within the proximal UCL ( open arrows ), consistent with chronic partial-thickness tearing. Note the absence of periligamentous edema. Mild focally increased signal near the sublime tubercle ( arrowhead ) was believed to be related to the patient’s symptoms. ( B ) Sequential flexed elbow valgus external rotation view images demonstrate chronic partial proximal UCL tearing ( solid arrows ).
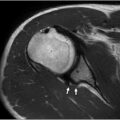
Coronal ( A ) and axial ( B ) T2 fat-saturated images of a 16 year old baseball player show an acute complete ulnar collateral ligament tear at the sublime tubercle. There is fluid ( solid arrows ) between the sublime tubercle and the distal ligament fibers. There is marrow edema subjacent to the distal attachment ( open arrow ). The proximal ligament fibers are heterogeneous with intermediate signal intensity ( open arrowhead ), and there is diffuse periligamentous edema and low-grade flexor–pronator mass strain ( solid arrowheads ).
UCL reconstruction (sometimes referred to as Tommy John surgery ) is the mainstay of operative treatment of patients in whom conservative management has failed and for those with high-grade UCL tears. The specifics of UCL reconstruction are beyond the scope of this article; however, the imaging features of the postoperative UCL warrant discussion.
The reconstruction graft is invariably thicker than the native UCL ( Fig. 14 ) and has a broader humeral attachment. Grafts may normally have increased intrasubstance fluid signal in the acute and subacute postoperative phases. This signal generally decreases in intensity over time as the graft matures but may persist in a subset of patients. , As such, partial graft tears ( Fig. 15 A, B ) provide a diagnostic challenge. The T sign of distal partial-thickness tears is not reliable for the postoperative UCL, as the graft attachment site is often more distal to the articular surface than the native ligament insertion site. Redundancy and laxity may be used as ancillary findings supporting the diagnosis of partial graft tears in borderline cases. Complete full-thickness graft tears are usually a more straightforward diagnosis, although scarring adjacent to full-thickness tears may make it difficult to distinguish them from high-grade partial-thickness tears ( Figs. 16–18 ). Fortunately, in the high-level athletes who usually comprise this population, high-grade partial-thickness and full-thickness graft tears are treated similarly. Other postoperative complications include hardware loosening at the graft attachment sites and medial epicondyle avulsion, which may occur due to the humeral tunnel(s) acting as a stress riser in throwing athletes ( Fig. 19 A, B ).
Coronal T2 fat-saturated image of a 25 year old major league baseball player in the early postoperative period after ulnar collateral ligament reconstruction. The graft fibers are contiguous ( arrow ). There is edema-like marrow signal in the humerus and mildly increased signal in the graft proximally ( arrowhead ), within the normal limits postoperatively.
( A ) Reformatted proton density 3D images of a 26 year old major league baseball pitcher 5 years post-ulnar collateral ligament (UCL) reconstruction. Long-axis images from posterior ( left ) to anterior ( right ) of the UCL graft show increased signal and ill-definition of the posterior fibers near the humeral tunnel ( solid arrow ). There is a more discrete partial-thickness tear in the mid-fibers with interstitial extension distally ( open arrow ). The anterior graft fibers appear intact ( solid arrowheads ). There is a low-grade flexor-pronator mass strain ( open arrowheads ). ( B ) Sagittal T2 fat-saturated images demonstrate partial tearing involving the posterior two-thirds of the graft near the humerus ( solid arrows ).
Related posts:
 Detailed Review of MSK Reporting and Data Systems
Detailed Review of MSK Reporting and Data Systems
 3 Dimensional MR Imaging of the Hand and Fingers
3 Dimensional MR Imaging of the Hand and Fingers
 High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
High-Resolution Peroneal Compartment Imaging at Ankle-2d and 3d MR Imaging
 High-Resolution Imaging of Knee Meniscus Anatomy and Tears
High-Resolution Imaging of Knee Meniscus Anatomy and Tears
 MR Neurography of Lower Extremity Sports-Related Nerve Injuries
MR Neurography of Lower Extremity Sports-Related Nerve Injuries
 Shoulder Impingement Syndromes: State of the Art Imaging
Shoulder Impingement Syndromes: State of the Art Imaging
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


