Management of sinonasal cancers is complex and tailored to histopathologic tumor characteristics and disease stage. Imaging plays a pivotal role in staging, largely determining surgical and/or medical treatment regimens. Here, we discuss staging criteria as it relates to head and neck anatomy as well as specific tumor types to help radiologists meaningfully contribute in a multidisciplinary setting.
Key points
-
•
Sinonasal cancers are of diverse histology but mostly indistinguishable imaging features with imaging predominantly used for tumor mapping and treatment planning.
-
•
Knowledge of the American Joint Committee on Cancer staging system is essential to accurately map the tumors.
-
•
Molecular distinguishing features that have been included in the new World Health Organization (WHO) classification also have implications for treatment and prognostication.
Abbreviations
| ACC | adenoid cystic carcinoma |
| AJCC | American Joint Committee on Cancer |
| BET | bromodomain and extraterminal domain |
| BPSS | biphenotypic sinonasal sarcoma |
| CLAC2 | chloride channel accessory-2 |
| DLBCL | diffuse large B cell lymphoma |
| EBV | Epstein–Barr virus |
| HPVMSCA | HPV-associated multiphenotypic sinonasal carcinoma |
| ITAC | intestinal type adenocacinoma |
| KSCC | keratinizing |
| NKSCC | nonkeratinizing |
| NKTL | natural killer (NK)/T cell lymphoma |
| Non-ITAC | non-intestinal type adenocacinoma |
| ON | olfactory neuroblastoma |
| SMARCB1 | SWI/SNF (SWIft/sucrose nonfermentable) related, matrix associated, actin dependent regulator of chromatin subfamily B, member 1 |
| SNCA | sinonasal cancers |
| SNF | sucrose nonfermentable |
| SNL | sinonasal lymphoma |
| SNMM | sinonasal malignant melanoma |
| SNSCC | Squamous cell carcinoma of the SNT |
| SNT | sinonasal tract |
| SNUC | sinonasal undifferentiated carcinoma |
| TIC | time-intensity curves |
Introduction
As imagers, our role in cancer management extends beyond pattern recognition and histologic diagnosis. We play a critical part in guiding treatment by providing essential insights that influence decisions regarding resectability and the selection of adjuvant therapies. To contribute meaningfully, and to better understand the perspectives of surgeons and oncologists, it is necessary to consult literature beyond standard radiology texts. Such interdisciplinary knowledge allows us to identify key factors that may significantly alter the course of treatment. The development and refinement of guidelines, such as the American Joint Committee on Cancer (AJCC) staging manual, exemplifies the importance of this multidisciplinary approach. In the following article, we will examine sinonasal cancers (SNCA) within the framework of current treatment guidelines, equipping readers to engage more effectively in collaborative decision-making.
Current treatment of sinonasal cancers
The surgical management of SNCA presents significant challenges due to the anatomic proximity to critical structures like the skull base and orbit. Traditionally, en bloc resection was preferred, which facilitated achievement of negative margins and minimized tumor seeding. , However, recent advances have led to a shift toward endoscopic approaches and piecemeal resection, ,,,,,,,, wherein any positive surgical margins are subsequently managed through limited revision surgery and adjuvant chemoradiation, ,, with the goal of preserving the quality of life. While some studies have reported slightly lower survival rates associated with this less-invasive approach, conclusive evidence remains elusive due to the rarity of SNCA.
An essential concept in the discussion of surgical management is the notion of resectability , which refers to the possibility of achieving a gross total resection with negative surgical margins. Tumors are generally deemed unresectable when they involve the orbital apex, dura mater, brain parenchyma, middle cranial fossa, cranial nerves other than the maxillary nerve (V2), nasopharynx, or clivus, forming the basis for their inclusion in the T4b category of AJCC staging. ,, Furthermore, tumors are considered surgically nontreatable in the presence of distant metastases or when unacceptable morbidity results from surgery.
The anatomic criteria outlined in the T staging ( Figs. 1–6 ) are useful in identifying nonsurgical cases—where palliative chemoradiation may be appropriate or early-stage cases—where achieving negative surgical margins is more feasible. In early-stage cases, definitive chemoradiation or radiation therapy alone may also be considered. Chemotherapy is also commonly used for induction or as a radiosensitizer during definitive treatment. , Adjuvant intensity-modulated radiation therapy is regarded as standard treatment for T2-T4 stage SNCA with proton radiation therapy, and carbon-ion radiation therapy being other competing options. ,,,
Maxillary sinus tumor. T1- confined to mucosa. T2- extends to hard palate and/or middle meatus with bone destruction.
T3 Maxillary sinus tumor can invade any of the following: posterior maxillary sinus wall, subcutaneous tissues, floor/medial orbital wall, pterygoid fossa, and ethmoid sinuses.
T4a maxillary sinus tumor can invade anterior orbital contents, skin of cheek, pterygoid plates, cribriform plate, sphenoid or frontal sinuses. T4b tumor can invade the orbital apex, dura, brain, middle cranial fossa, cranial nerves other than V2, nasopharynx or clivus.
Ethmoid/nasal cavity tumor. T1- restricted to one subsite ± bone erosion. T2- two subsites in a single region or extension to adjacent region in the nasoethmoid complex ± bone erosion.
Ethmoid/nasal cavity tumor. T3 can invade medial wall/floor of orbit, maxillary sinus, palate or cribriform plate. T4a can invade anterior orbital contents, skin of nose/cheek, minimally into anterior cranial fossa, pterygoid plates, sphenoid or frontal sinus while T4b can invade the orbital apex, dura, brain, middle cranial fossa, cranial nerves other than V2, nasopharynx and clivus.
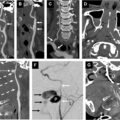
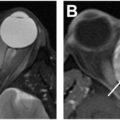
Sinonasal malignancy T staging landmarks. Maxillary sinus T3 disease ( upper panel left ) can involve the bone of maxillary sinus posterior wall ( A , arrow ), subcutaneous tissues ( B , arrow ), floor or medial wall of orbit ( C , arrow ), pterygopalatine fossa ( B , arrowhead ), or ethmoid sinus ( D , arrow ). Nasal cavity/ethmoid sinus T3 disease ( upper panel right ) can involve the maxillary sinus ( E , arrow ), medial wall of the orbit ( F , arrow ), palate ( F , arrowhead ), or cribriform plate ( F , curved arrow ). T4 disease is subdivided into T4a ( middle panel ), which can involve the anterior orbital contents ( G , arrow ), minimally into the anterior cranial fossa ( G , arrowhead ), skin of nose or cheek ( H , arrow ), pterygoid plates ( I , arrow ), sphenoid sinus ( J , arrow ) or frontal sinus; and T4b ( lower panel ), which can involve the orbital apex ( K ), dura ( L ), middle cranial fossa ( M ), cranial nerves other than V2 ( N , arrow on V3 division), nasopharynx ( O , arrow ), or clivus ( O , arrowhead ).
Lymphadenopathy can influence treatment strategy, with neck dissection typically offered to node-positive patients undergoing curative treatment. , The management of node-negative patients remains a subject of ongoing debate, and decision to pursue elective treatment of nodal disease is largely guided by the biological behavior of the tumor.
This highlights the critical role of accurate tumor staging and underscores the importance of delineating specific anatomic features that define each T stage, since precise staging guides therapeutic decision-making and influences prognostication. The choice of therapy ultimately depends on several tumor-specific factors, including histologic subtype, grade, genetic alterations, and molecular profile and the disease stage.
Classification and WHO fifth edition update
Besides tumor stage and resectability, there is a growing emphasis on incorporating tumor histopathology and molecular profiling to guide treatment and refine prognostication. , For instance, several distinct tumor entities have recently been separated from sinonasal undifferentiated carcinoma (SNUC). , These newly defined subgroups exhibit varying degrees of aggressiveness and prognostic outcomes. Notably, tumors harboring isocitrate dehydorgenase (IDH) mutations tend to demonstrate more favorable overall survival, whereas SWI/SNF (smad wing for transcriptional activation [SWIft]/sucrose nonfermentable) related, matrix associated, actin dependent regulator of chromatin subfamily B, member 1 (SMARCB1) deficient carcinomas are characterized by significantly poorer disease-free and overall survival. ,
Another recently recognized entity, human papilloma virus (HPV)-associated multiphenotypic sinonasal carcinoma (HPVMSCA)—previously referred to as HPV-related carcinoma with adenoid cystic-like features—mimics adenoid cystic carcinoma (ACC) on routine histologic examination. However, unlike true ACC, it demonstrates a markedly lower tendency for perineural tumor spread and is associated with a significantly more favorable prognosis. ,
DEK-AFF2 gene fusions have been identified in a subset of squamous cell carcinomas that exhibit papilloma-like features on histologic examination. Despite their deceptively benign appearance, these tumors are associated with an aggressive clinical course, characterized by a high frequency of local recurrences and distant metastases. ,
In sinonasal adenocarcinomas, gene methylation has been implicated in the differential development of less aggressive tumor phenotypes. Notably, positive p16 protein expression has been associated with shorter overall survival, suggesting a potential prognostic role. Additionally, absence of annexin A2 expression—identified using similar molecular techniques—has been correlated with the aggressive mucinous subtype, which is linked to poorer survival outcomes. , Furthermore, several potentially actionable genetic alterations have been identified, prompting ongoing research into targeted therapy, including the use of immunotherapy and immune checkpoint inhibitors. , Genetic profile can also be used to differentiate tumors. For example, several genes differentiate SNUC from squamous cell carcinomas (SCCs), including the expression of human chloride channel accessory-2 (CLAC2) gene which is markedly different between the 2. ,
Given the growing potential of targeted therapies, the latest edition of the WHO classification ( Box 1 ) has incorporated a range of genetic and molecular profiles. Notably, entities such as SWI/SNF complex-deficient sinonasal carcinoma, nuclear protein testis (NUT) carcinoma, and HPVMSCA have been formally recognized based on their distinct molecular characteristics. In contrast to previous editions, the latest classification excludes hematolymphoid, melanocytic, neuroendocrine, and soft tissue tumors, as these are not specific to the sinonasal tract (SNT) and are better classified according to broader criteria.
Box 1
Fifth edition WHO malignant tumors of the sinonasal tract
-
Epithelial malignancies
-
•
Squamous cell carcinoma
-
○
Keratinizing
-
○
Nonkeratinizing
-
○
-
•
SWI/SNF complex-deficient sinonasal carcinoma
-
•
NUT carcinoma
-
•
Sinonasal lymphoepithelial carcinoma
-
•
SNUC
-
•
HPVMSCA
-
•
Teratocarcinosarcoma
-
•
Adenocarcinoma
-
○
Intestinal type
-
○
Nonintestinal type
-
○
-
•
-
Mesenchymal malignancies
-
•
Chordoma
-
•
BPSS
-
•
-
Other tumors
-
•
ON
-
•
Sinonasal ameloblastoma
-
•
Imaging and tumor mapping
CT and MR imaging are complementary in the imaging of SNCA. CT is valuable for precise depiction of osseus erosionI; MR imaging excels in soft tissue evaluation, distinguishing tumor tissue from retained secretions within the paranasal sinuses, detecting orbital and intracranial extension, brain parenchymal invasion, and perineural tumor spread.
For assessment of lymphadenopathy, both CT and MR imaging can be employed effectively. Distant metastases, more common in aggressive histologic subtypes such as SNUCs and NUT carcinomas, are best evaluated using PET imaging with comprehensive whole-body assessment and metabolic characterization. MR imaging is typically the preferred modality for follow-up, owing to its superior soft tissue contrast and sensitivity in detecting residual or recurrent disease. CT and PET imaging are generally reserved for problem-solving, particularly in cases where MR imaging findings are inconclusive or when there is a need to evaluate osseous changes or distant metastases ( Box 2 ).
Box 2
Tumor mapping audit sheet
-
Differentiate tumor from secretions
-
Multisite involvement (relevant for ethmoid/nasal cavity staging)
-
Multisinus involvement
-
Bone erosion (hard palate, pterygoid plates, and clivus)
-
Orbit involvement (medial wall/floor vs apex)
-
Intracranial extension (cribriform plate vs dura and brain)
-
Involvement of subcutaneous tissues and skin
-
Perineural tumor
-
Lymphadenopathy (Levels I-III and retropharyngeal lymph nodes [RPN])
-
Distant metastasis
As discussed earlier, treatment planning greatly depends on staging of SNCA, where imaging plays a pivotal role in tumor mapping. , Another key role of imaging is differentiating malignant tumors from benign entities ( Box 3 ). Benign lesions typically present with smooth, well-defined margins, displacement rather than invasion of adjacent tissue planes, bone remodeling rather than destruction, and high signal intensity on T2-weighted MR imaging. In contrast, malignant tumors often exhibit infiltrative margins, invasion of tissue planes, bone destruction, and relative T2-hypointensity. Benign inflammatory polyps and mucoceles tend to be nonenhancing or exhibit only marginal enhancement, whereas malignant tumors typically demonstrate internal or heterogeneous enhancement. ,
Box 3
Imaging features suggestive of malignancy
-
Infiltrative margins
-
Heterogeneous enhancement with necrosis
-
Low MR imaging T2 signal
-
Decreased diffusivity
-
Bone erosion
-
Adjacent tissue involvement
-
Perineural tumor spread
-
Metastasis
Benign lesions generally demonstrate high diffusivity, while malignant, hypercellular tumors show restricted diffusion. Malignant tumors have a lower ADC, higher kurtosis, lower diffusion coefficient, and high perfusion fraction compared to benign lesions. ,, Dynamic contrast-enhanced MR imaging generates time-intensity curves (TICs), which are analyzed for metrics such as time to maximum enhancement and peak enhancement (Tpeak). The shape of the TIC provides insight into tumor behavior. A persistent enhancement pattern suggests a benign lesion, whereas a washout pattern is indicative of malignancy.
Staging sinonasal cancers
The AJCC delineates staging criteria for SNCA carcinomas arising from the epithelial lining based on their primary site of origin—the maxillary sinus, ethmoid sinus, and/or nasal cavity. AJCC staging system does not apply to nonepithelial tumors such as lymphomas, sarcomas, or mucosal melanomas, which follow distinct staging systems.
The nasal cavity is subdivided into 4 distinct anatomic regions: the nasal septum, nasal cavity floor, lateral wall, and the region extending from the edge of the naris to the mucocutaneous junction. Careful assessment of these subsites is critical, as tumor extension beyond a single subsite into 2 or more subsites is designated as T2 in nasal cavity and ethmoid sinus carcinoma ( Table 1 ).
Table 1
American Joint Committee on CancerT-staging qualifiers for epithelial sinonasal cancers
| Organ Involvement | Maxillary Sinus | Ethmoid Sinus and Nasal Cavity | |
|---|---|---|---|
| Index site | Limited to sinus mucosa/single subsite, no bone erosion | T1 | T1 |
| Limited to sinus mucosa/single subsite, with bone erosion | T2 | T1 | |
| Two subsites in a single region or adjacent region in the nasoethmoidal complex | Does not apply | T2 | |
| Maxillary sinus | Remains T2 unless there is involvement of posterior wall | T3 | |
| Posterior maxillary sinus wall | T3 | T3 | |
| Ethmoid sinus | T3 | Depends on primary site | |
| Bone erosion | Hard palate | T2 | T3 |
| Middle meatus | T2 | Depends on primary site | |
| Cribriform plate | T4a | T3 | |
| Medial wall or floor of orbit | T3 | T3 | |
| Pterygoid plate | T4a | T4a | |
| Clivus | T4b | T4b | |
| Adjacent region | Sphenoid or frontal sinus | T4a | T4a |
| Nasopharynx | T4b | T4b | |
| Orbit | Anterior orbital contents | T4a | T4a |
| Orbital apex | T4b | T4b | |
| Skin and subcutaneous tissue | Subcutaneous tissue | T3 | |
| Skin of nose/cheek | T4a | T4a | |
| Intracranial extension | Minimal extension into anterior cranial fossa | T4a | T4a |
| Extension into middle cranial fossa | T4b | T4b | |
| Dura, brain, cranial nerves other than V2 | T4b | T4b | |
The T category in SNCA is defined primarily by the extent of invasion into specific anatomic structures, rather than by tumor size, reflecting the critical impact of local extension on both surgical resectability and prognosis. For example, in maxillary sinus tumors, osseous erosion is typically classified as T2 disease (see Table 1 , see Fig. 1 ). However, posterior extension involving the posterior wall of the maxillary sinus or the pterygoid plates is considered T3 and T4 disease (see Table 1 , Figs. 2, 3 and 6 ), respectively, since posterior involvement significantly reduces the likelihood of tumor free surgical margins due to the tumor’s proximity to critical structures. Similarly, invasion of the medial orbital wall or orbital floor is classified as T3 disease (see Table 1 , see Figs. 2,5,6 ) reflecting intermediate local extension. Involvement of the anterior orbital contents—such as the extraocular muscles or orbital fat—is categorized as T4a, indicating moderately advanced disease with potential for resection. In contrast, extension to the orbital apex, a region housing critical neurovascular structures, represents T4b disease, the most advanced T category, often associated with poor surgical accessibility and limited curative options.
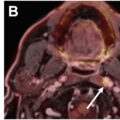
Although relatively uncommon, nodal involvement significantly worsens prognosis and typically affects lymph node levels I–III and the retropharyngeal chains. Consequently, stage IV ( Fig. 7 ) disease encompasses cases with ipsilateral nodal involvement greater than 3 cm or multiple nodes involved on either side, regardless of the T classification. Consistent with other cancers, the presence of extranodal extension is designated as the most advanced nodal stage (N3b), irrespective of lymph node size.
Nodal and distant metastases in poorly differentiated SNSCC. Coronal STIR ( A ) and T1W + C ( B ) MR imaging shows an infiltrative mass centered in the left nasal cavity ( arrows ). Axial T1W + C MR imaging ( C ) of the brain shows a right temporal lobe metastasis ( arrow ). Coronal ( D ) and axial ( E ) Fluorodeoxygluose-Positron emission tomography (FDG PET)/CT shows additional distant metastases of the bones ( arrows ), lung ( arrowhead ), mediastinal/hilar lymph nodes ( curved arrows ), and left cervical level IIA lymph node ( perpendicular arrow ).
Epithelial malignancies
Squamous Cell Carcinoma
Squamous cell carcinoma of the SNT (SNSCC) is classically defined as a malignant epithelial neoplasm arising from the surface epithelium, characterized by squamous differentiation, although it truly represents a biologically heterogeneous group of tumors with varying clinical and pathologic features. ,,
A recent US National Cancer Institute’s Surveillance, Epidemiology, and End Results database reported an incidence of 0.32 new cases per 100,000 individuals per year, with a steady decline of approximately 2.6% annually over the past 3 decades. The disease shows a male-to-female incidence ratio of 2.3:1, and nearly 80% of patients are 55 years of age or older at diagnosis.
SNSCC is the most prevalent malignant neoplasm of the SNT (50%–60% of all SNCA), most frequently affects the maxillary sinus (60%), followed by the nasal cavity (25%) and the ethmoidal complex (15%). SNSCCs originating in the maxillary sinus tend to exhibit higher incidence of nodal involvement compared to those arising in the nasoethmoidal complex, likely attributable to differences in lymphatic drainage.
SNSCC is histologically classified into keratinizing (KSCC, 50%) and nonkeratinizing (NKSCC, 30%) subtypes, and the remaining other morphologic variants (20%), each characterized by distinct histopathological features.
Approximately 20% to 25% of SNSCCs are HPV-positive, the majority being the NKSCC subtype, which often display histomorphological features similar to those of HPV-associated SCCs of the oropharynx. Emerging evidence suggests that HPV-positive SNSCCs may be associated with a more favorable clinical outcome compared to their HPV-negative counterparts. ,,
A distinct subset of NKSCCs has been found to harbor the DEK-AFF2 gene fusion as discussed above. ,, Despite their somewhat indolent histologic appearance, DEK-AFF2-rearranged NKSCCs have been linked to high rates of local recurrence, therefore requiring careful clinical monitoring. ,,
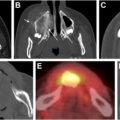
SNSCCs typically present with a nonspecific radiologic appearance ( Fig. 8 ) that closely resembles other epithelial malignancies often demonstrating heterogeneous signal characteristics, appearing hypointense to isointense on T1-weighted sequences and variable, though frequently low signal intensity on T2-weighted sequences. They exhibit avid contrast enhancement with frequent areas of necrosis, adjacent bone destruction, and invasion of surrounding soft tissues. ,
SNSCC. Axial STIR ( A ), axial ( B ) and coronal ( C – E ) T1W + C MR imaging images show a large, destructive, enhancing, STIR hypointense left maxillary sinus mass ( A–C , arrows ) extending into the cheek subcutaneous fat ( B , arrowhead ) and infratemporal fossa ( B , curved arrow ). Abnormal enhancement along the maxillary (V2) ( C, D , arrowheads ) and mandibular divisions (V3) ( E , arrow ) of the left trigeminal nerve suggests perineural tumor spread.
NUT Carcinoma
NUT carcinoma, previously known as nuclear protein testis (NUT) midline carcinoma, is a rare and highly aggressive malignancy defined by chromosomal rearrangements involving the NUTM1 gene, most commonly resulting in a fusion with bromodoamin containing protien 4 (BRD4) on chromosome 19p13.1. This fusion leads to the formation of the BRD4-NUTM1 oncoprotein, which disrupts normal cellular differentiation and promotes uncontrolled proliferation. ,,
NUT predominantly affects midline anatomic structures, including the head and neck region (SNT), thorax, and, less frequently, the testis. Patients can be of any age, but there is a predilection for adolescents and young adults. ,,
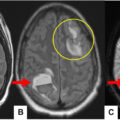
Imaging studies typically reveal a large, aggressive mass with invasion into adjacent orbit and anterior cranial fossa ( Fig. 9 ). On CT, the tumor may appear as a soft-tissue mass with possible faint mineralization. MR imaging often shows a heterogeneous lesion with low signal intensity on T1-weighted images, high signal intensity on T2-weighted images, and heterogeneous enhancement. , Histologically, it is characterized by poorly differentiated carcinoma with abrupt squamous differentiation. ,,