(1)
Radiology Department Beijing You’an Hospital, Capital Medical University, Beijing, People’s Republic of China
16.2.1 Pathogens and Pathogenesis
16.2.2 Pathophysiological Basis
16.2.3 Clinical Symptoms and Signs
16.2.5 Imaging Demonstrations
16.2.6 Discussions
16.2.7 Criteria for the Diagnosis
16.2.8 Differential Diagnosis
16.3.1 Pathogen and Pathogenesis
16.3.2 Pathophysiological Basis
16.3.3 Clinical Symptoms and Signs
16.3.5 Imaging Demonstrations
16.3.6 Discussions
16.3.7 Criteria for the Diagnosis
16.3.8 Differential Diagnosis
16.4.1 Pathogen and Pathogenesis
16.4.2 Clinical Symptoms and Signs
16.4.4 Imaging Demonstrations
16.4.5 Criteria for the Diagnosis
16.4.6 Differential Diagnosis
16.5.1 Pathogen and Pathogenesis
16.5.2 Pathophysiological Basis
16.5.3 Clinical Symptoms and Signs
16.5.5 Imaging Demonstrations
16.5.6 Diagnostic Criteria
16.5.7 Differential Diagnosis
Abstract
AIDS patients often develop otorhinolaryngological diseases as Marcuser and Sooy [9] reported in 1985 that 165 cases among 399 AIDS patients (41 %) have cranial and cervical symptoms, including oral and pharyngeal KS, candida infection and the most commonly found nasal sinusitis.
Keywords
HIV/AIDS related thyromegalyHIV/AIDS related cervical lymphoid tuberculosisHIV/AIDS related neoplasm16.1 An Overview of HIV/AIDS Related Neck Diseases
AIDS patients often develop otorhinolaryngological diseases as Marcuser and Sooy [9] reported in 1985 that 165 cases among 399 AIDS patients (41 %) have cranial and cervical symptoms, including oral and pharyngeal KS, candida infection and the most commonly found nasal sinusitis.
HIV/AIDS related lymphoid tuberculosis results in cervical lymphadenectasis. The swollen lymph-node cells are exhausted to necrosis and liquefaction.
HIV/AIDS related otorhinolaryngological diseases include suppurative otitis externa, otitis media, tonsillitis, chronic pharyngitis and sinusitis caused by pathogens of anaerobes, candida, cryptococcus and herpesvirus. All these opportunistic infections are manifestations of compromised immunity.
In terms of HIV/AIDS related thyroid and parathyroid diseases, it is reported that patients with HIV infection have thyroid infections by pathogens of pneumocystis carinii, cryptococcus, CMV and toxoplasma. Thyroiditis can cause functional morphological changes and it has been reported that patients with advanced stage of HIV infection complicated by lymphoma have accompanying hypercalcemia and serum PTH inhibition yet no reports about thyroid lesions in the cases of hypercalcemia.
16.2 HIV/AIDS Related Thyromegaly
16.2.1 Pathogens and Pathogenesis
AIDS can indirectly or directly involve all the systems in the human body and endocrine system is not an exception. HIV/AIDS induced infections, non-specific inflammations, hemorrhage and cancer all wreck damages to the endocrine tissues. Antibodies and cytokines produced by acute and chronic complications such as tumor necrosis factor (TNF), IF-1 and IF-N may interfere functions of the endocrine glands. Medications for their treatment may also impose adverse effects on the endocrine tissues. For instance, Ketoconazole for fungal infections can inhibit synthesis of cortisol and testosterone; Rifampicin against tuberculosis can promote cortisol catabolism; Pentamidine for PCP can result in damages to the islet beta cell. Endocrine dysfunction of AIDS patients vary with severities of the particular conditions and its occurrence may be due to conditions ranging from slightly abnormal hormonal secretions and metabolism to complete failure of an endocrine gland.
It has consistently been reported that changes of thyroid functions and morphology occur in patients with AIDS and the related research has been attracted increasingly focused attention. Asymptomatic patients with AIDS predominantly have normal thyroid function, and increased levels of T3 and T4 are rarely found due to increases of TBG concentration of unknown reasons. However, with progression of AIDS and decrease of TBG level, serum levels of T3 and T4 decline gradually as T4 transforms into T3 in the peripheral tissues and TSH secretion decreases. In advanced stage of AIDS, the patients may sustain slight decrease of HSH level. The changes of thyroid hormone level in patients with AIDS are similar to those with other general chronic diseases. However, the decrease of T3 level in AIDS patients is not as obvious as patients with other general chronic diseases in frequency and severity. There have also been reports about diffuse thyroid enlargement and hyperthyroidism in a few cases of AIDS and it has been speculated in these reports that the compromised immunity of AIDS patients causes immune damages to the thyroid and further causes hyperthyroidism/hypothyroidism and its morphological enlargement. The morphological and structural changes of enlarged thyroid can be detected by the diagnostic imaging.
The causes of HIV/AIDS related thyromegaly remains unclear. It is generally believed that the clinically defined causes of thyromegaly are also applicable to HIV/AIDS related thyromegaly. However, the underlying relations between these causes and AIDS remain elusive.
16.2.1.1 Iodine Deficiency and Thyromegaly Caused by Excessive Iodine
Iodine deficiency is the main cause of endemic thyromegaly, mostly found in inlands and mountain areas with a high altitude far away from oceans. Increased demand for thyroxin in periods of puberty, pregnancy, lactation and menopause as well as a result of mental stimulation and traumas can lead to relative iodine deficiency. In cases of environmental iodine deficiency or decreased serum inorganic iodine concentration, hyperplasia of the thyroid tissues occurs to boost its function of iodine intake. Therefore, the thyroid can take in enough iodine from blood under low iodine condition to ensure synthesis of enough thyroid hormones for physiological demand of the body tissues. However, in cases of severe deficiency of iodine, this compensation mechanism can not maintain normal thyroid functions so the thyroid preferably synthesizes and secretes T3 which needs less iodine but has stronger activity and T4 synthesis decreases. Moreover, as T4 concentration is an essential cause for pituitary stimulation to produce TSH, decreased T4 concentration increases the pituitary stimulation to produce more TSH which further aggravates thyroid hyperplasia and enlargement. Contrarily, for cases with long-term excessive intake of iodine, excessive inorganic iodine ions in the thyroid tissues can impede iodine organizing process, resulting in decreased synthesis of thyroxin. Additionally, thyroxin release inhibition by abundant iodine contributes to further deficiency of blood thyroxin, which increases TSH synthesis and secretion and causes thyromegaly.
Clinical observation reveals that blood T3 and T4 levels decrease significantly with accompanying decrease of sex hormones. According to the above-mentioned mechanism, decreases of T3 and T4 levels can likewise lead to thyromegaly. Moreover, T3 and T4 level are associated with the survival rate of AIDS patients. The decreases of T3 and T4 levels are the accurate predictor for occurrence of death in AIDS patients.
16.2.1.2 Substances Causing Thyromegaly
It has been demonstrated that some food and drugs may be of certain relations with thyromegaly. For instances, long-term intake of cabbages in a large quantity can result in thyromegaly. It has been found by researchers that organic cyanides in cabbages can interfere in iodide oxidation to affect the synthesis of the thyroid hormones, therefore leading to compensatory thyroid enlargement. Prolonged oral administration of some medicines as potassium cyanide, potassium perchlorate, Aminosalicylic acid, phenyl-butazone, Sulfanilamide and Thioureas can hinder the synthesis of thyroid hormones and inhibit their releases. Consequently, thyroxin in blood decreases and TSH level increases, lead to thyromegaly. AIDS patients are commonly treated with various combinations of drugs. It cannot be excluded that some medicines have impacts on synthesis and release of thyroxin, leading to thyromegaly.
16.2.1.3 Congenital Defects in Thyroid Hormone Synthesis
Synthesis of thyroid hormones cannot be completed without the catalyses of various specialized enzymes. AIDS patients probably have congenital defects in thyroid hormone synthesis. The related symptoms are prone to be clinically manifested in the stage of AIDS.
16.2.1.4 Thyroid Immune Damage due to the Compromised Immunity
It has been reported that AIDS patients may be complicated by hyperthyroidism or hypothyroidism. Observation of thyroid hormone level and immunity suggests that immunological damages to the thyroid tissues may occur but its underlying mechanism has not be definitively reported.
16.2.2 Pathophysiological Basis
The lesion of HIV/AIDS related thyromegaly is diffuse and soft, with no nodules and with diffuse enlargement of the volume including the both lateral lobes and isthmus. Cases with persistent long-term thyromegaly may have multiple nodules, with various sizes, heterogeneous density and possibly formation into cysts, sometimes with accompanying hemorrhage.
16.2.3 Clinical Symptoms and Signs
Thyromegaly complicating HIV/AIDS has principal demonstrations of diffuse enlargement of the thyroid, being soft and with no nodules by palpitation. Thyromegaly can be graded into 3° according to the findings by palpitation: degree I—invisible but palpable enlargement of the thyroid; degree II—visible and palpable enlargement of the thyroid but the thyroid being within sternocleidomastoid; degree III—the enlarged thyroid exceeding the lateral margin of sternocleidomastoid. Diffuse thyroid enlargement rarely results in symptoms of local compression. In the nodular stage, nodules of different sizes occur to compress the trachea, resulting in dyspnea. Or the nodules compress the recurrent laryngeal nerve, resulting in coarse sound. Changes of thyroid functions occur in the advanced stage of AIDS, commonly decreased thyroid functions but with rare reports of hyperthyroidism. The corresponding symptoms of hypothyroidism/hyperthyroidism are concurrent with the clinical symptoms of HIV/AIDS, presenting great difficulty for the differential diagnosis. Therefore, diagnosis of thyroid functions should be based on the blood T3 and T4 levels.
16.2.4 Examinations and Their Selection
Nuclear imaging and ultrasound are important examination methods for thyroid diseases. ECT of thyroid mainly demonstrates iodine intake rate by the thyroid, based on which the differential diagnosis of nodular lesions can be made. Ultrasound can provide a detailed assessment on the shapes and sizes of the thyroid and can sensitively detect the thyroid nodules, calcification and cysts as well as the blood supply of the lesions. CT scanning is commonly applied for the assessment of the thyroid, demonstrating the size, shape and density of the thyroid as well as the nodules, cysts, bleeding and calcification in it. Concerning the invasion and extension of the lesions to the surrounding tissues, CT scanning plays an important role. For instance, in cases of giant thyromegaly compressing the trachea, CT scanning can show the mass extension posterior to the trachea or superior to the mediastinum as well as the compressed changes of the trachea.
16.2.5 Imaging Demonstrations
16.2.5.1 Nuclear Imaging Demonstrations
Nuclear imaging demonstrates homogeneous radioactive distribution of the bilateral lobes that are similar to the normal thyroid or homogeneous increase of radioactive concentration. For cases with nodules, the demonstrations include local defects of radioactive distribution in the thyroid parenchyma, being worm-eaten liked.
16.2.5.2 Ultrasound Demonstrations
Ultrasound demonstrates homogeneous enlargement of thyroid parenchyma, with its severity being related to the course and severity of the illness. The interior echo is normal, moderate and homogeneous, with occasionally scattering cystic nodules in homogeneous non-echo areas with smooth borderlines. CDFI generally demonstrates no obvious abnormalities.
16.2.5.3 CT Scanning Demonstrations
CT scanning demonstrates diffuse enlargement of the thyroid with symmetric enlargement of the bilateral lobes and isthmus. The tissues density may be normal but commonly decreases. It is likely to be diffuse scattering spot liked lower density shadows in the thyroid. By enhanced scanning, there is obvious homogeneous enhancement with clearly defined borderlines. The highly enlarged thyroid can compress its surrounding tissues for their morphological changes. The compressed trachea can be narrowed and prolonged. For cases with nodular thyromegaly, there are multiple round shaped low density areas in the thyroid parenchyma, with different sizes and clearly defined borderlines. Enhanced scanning demonstrates the lower enhancement of the thyroid than its surrounding parenchyma. No obvious enhancement of the foci indicates formation of cysts.
16.2.5.4 MR Imaging Demonstrations
MR imaging demonstrates the same morphological changes. Enlarged thyroid parenchyma shows homogeneous moderate high signal by T2WI and homogenous equal or slightly high signal by T1WI based on the varying protein concentrations in the parenchyma. The cysts show regional higher signal by T2WI and relatively lower signal by T1WI with smooth borderlines. The enlarged nodules are demonstrated as moderate high signal that is slightly lower than the peripheral parenchyma by T2WI, and regional high signal by T1WI with smooth borderlines.
Case Study 1
A female patient aged 49 years with AIDS was confirmatively diagnosed by CDC. The onset of symptoms was accidentally found in 2001. The mass was located in the right anterior cervical thyroid which could move upward and downward along with swallowing. Her CD4 T cell count was 37/μl.
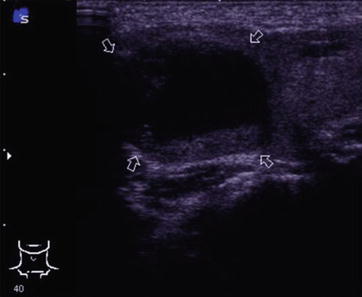
Fig. 16.1
HIV/AIDS related thyroid adenoma (follicular adenoma). Color ultrasonography demonstrates cystic parenchymal mass in size of 45 × 35 mm in the right thyroid lobe (arrows), with clearly defined borderline, predominant liquid low echo inside with intervals of strip liked slightly high echo. CDFI demonstrates unobvious blood flow signal in and surrounding the mass
Case Study 2
A female patient aged 53 years with AIDS was confirmatively diagnosed by CDC. The onset of symptoms was in 2003. She had fever and was detected with nodules in the left thyroid lobe by cervical examinations. Her CD4 T cell count was 37/μl.
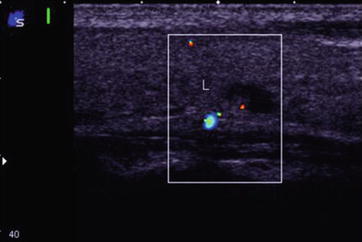
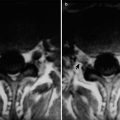
Fig. 16.2
HIV/AIDS related thyroid adenoma (papillary adenoma). Color ultrasonography demonstrates a cystic parenchymal low echo nodule in the left thyroid lobe. The nodule is clearly defined in size of 12 × 6 mm with liquid low density inside and a papillary adhesive wall with slightly high echo. CDFI demonstrates papillary blood flow signals with slightly high echo
16.2.6 Discussions
Occurrence of thyroid diseases in AIDS patients is increasingly high in recent years, and thyroid adenoma is the most commonly seen disease. Clinically, thyroid adenoma is common, with a high occurrence, which mostly has benign lesions and rarely malignancies. The pathogenesis remains unclear and pathological changes include thyroid follicular hyperplasia and enlargement of thyroid tissues. The begin lesions are soft in texture while the malignant ones are hard. The benign cervical mass is commonly singular, with slow growth. The large one may compress its surrounding tissues. The mass may move upward and downward along with swallowing and is smooth, soft, round or oval in shape, which may cause hyperthyroidism. Conclusively, the principal pathogenic causes include excessive estrogen induced by endocrine disorder, excessive iodine intake and mental conditions.
Pathological classification of thyroid adenoma
1.
Follicular adenoma
The most commonly benign thyroid tumors which can further divided into the following five types: (1) Embryonal adenoma; (2) Fetal adenoma; (3) Colloidal adenoma, also known as Giant follicular adenoma; (4) Simple adenoma; (5) Acidophilic adenoma.
2.
Papillary adenoma
Papillary adenomas are rarely benign and mostly cystic, therefore they are also known as papillary cystadenoma. Thyroid adenoma with papillary structures is most likely to develop into malignancy.
3.
Atypical adenoma
It is relatively rare with complete capsule of the tumor and being hard in texture
4.
Thyroid cyst
It can be classified into colloid cyst, serous cyst, necrotic cyst and hemorrhagic cyst according to its contents.
5.
Autonomous hyperfunctioning thyroid adenoma
In the neoplasm parenchyma, foci of old hemorrhage necrosis, cystic changes, hyaline change, fibrosis and calcification can be found. The tumor tissues are clearly defined, commonly with atrophy of its surrounding thyroid tissues.
6.
Toxic thyroid adenoma
Toxic thyroid adenoma shows enhanced function of thyroid to synthesize and secrete large amount of thyroid hormones resulting in hyperthyroidism. Toxic thyroid adenoma is mostly found in females aged 30–40 years. The adenoma is usually singular and multiple in rare cases. The patients have symptoms of hyperthyroidism and by physical examinations thyroid nodules are commonly found, generally being large in size of several centimeters. Serum T3 and T4 levels increase, especially significant T3 level increase. Thyroid scanning demonstrates that the nodules are hot nodules but radioactive isotopes usually are deficient or decreased in the peripheral thyroid tissues.
16.2.7 Criteria for the Diagnosis
The relationship between HIV infection and thyromegaly remains unclear; hence the diagnosis of HIV/AIDS related thyromegaly basically depends on diagnosis of HIV infection in combination with diagnosis of thyromegaly. In addition to the understanding of pathological and morphological changes of the tissues, a basic illness history of HIV infection should also be taken into account as well as the blood test results, such as CD4 T count and its ratio to CD8 T count as well as serum HIV antibody positive. Meanwhile, thyromegaly caused by other factors should be differentially diagnosed, especially autoimmune induced thyromegaly (Hashimoto thyroiditis).
16.2.8 Differential Diagnosis
HIV/AIDS related thyromegaly should be differentially diagnosed from following diseases:
16.2.8.1 Diffuse Thyromegaly
Hyperplasia may be caused by dietary iodine deficiency or hyperthyroidism or inflammation. The diffusely enlarged thyroid commonly extends to retrosternal or other areas. CT scanning demonstrates CT values of the thyroid tissues mostly above 70 Hu due to abundant contents of iodine. Tracheas and brachiocephalic blood vessels are compressed for migration and deformation and the superior vena cava is compressed for secondary venectasia. For cases with degeneration, it may demonstrate flaky calcification and cystic changes. By enhanced scanning, the thyroid tissues show enhancement, with no enhancement of cysts and rare enhancement of the degenerating lesions. Differential diagnosis of HIV/AIDS related thyromegaly from simple thyromegaly is difficult. For cases with diffuse thyromegaly complicating HIV/AIDS, the common causes of simple thyromegaly should be firstly excluded for the diagnosis of HIV/AIDS related thyromegaly.
16.2.8.2 Hashimoto Thyroiditis
It has manifestations of diffuse enlargement of the thyroid with infiltration toward the peripheral area. The enlargement is lobulated with unclearly defined borderlines and a density generally lower than normal thyroid tissues but close to the peripheral muscular tissues. It can be complicated by calcification and cystic changes. After intravenous injection of reagent, there is heterogeneous enhancement. Generally, the illness course is long. Based on the clinical manifestations and case history, its diagnosis can be made. Only by CT scanning, the differential diagnosis from neoplasms is difficult.
16.2.8.3 Thyroid Carcinoma
Differential diagnosis of obvious thyroid carcinoma is not necessary. Thyroid carcinoma initially shows local nodules in thyroid parenchyma, which should be differentiated from nodules manifested in cases of HIV/AIDS related thyromegaly.
Thyroid carcinoma can be divided into five types: papillary, follicular, encephaloid, giant cell and Hürthle cell. CT scanning can define the range of the lesions as well as lymphoid metastases. In terms of thyroid masses, there are no reliable signs to differentiate the benign from the malignant. For cases with regional lymphadenectasis, recurrent laryngeal nerve paralysis and injuries of thyroid cartilage or other laryngeal cartilages, it is facilitative for the diagnosis of malignancy. Calcification is not the evidence for the differentiation of the benign from the malignant because calcification occurs in cases of benign tumors. Nuclear imaging can roughly evaluate the biological activity of thyroid nodules, which facilitates the differential diagnosis. Thyroid carcinoma commonly shows cold nodules, mostly common with adenoma hyperplasia which can be cystic or parenchymal. Only 20 % nodules are malignant.
16.3 HIV/AIDS Related Cervical Lymphoid Tuberculosis
16.3.1 Pathogen and Pathogenesis
HIV/AIDS related cervical lymphoid tuberculosis can be classified into primary and secondary.
16.3.1.1 Primary Lymphoid Tuberculosis
Cervical lymphoid tuberculosis is a part of primary tuberculosis infection. Primary infection foci can be caused by invasion of M. Tuberculosis via upper respiratory tract or the oral cavity and nasopharynx. The most common location of the primary infection is the tonsil. The infection further spreads to the cervical superficial or deep lymph nodes or submandibular lymph nodes along lymph vessels, with possible involvement of preauricular and retroauricular lymph nodes. At this time of infection, the primary foci may have been absorbed gradually. But lymphoid tuberculosis may progress into cold abscess or ulcer.
16.3.1.2 Secondary Lymphoid Tuberculosis
After the primary tuberculosis or during the progression of secondary tuberculosis, tuberculosis invades the cervical lymph nodes via blood-borne transmission. The involved cervical lymph nodes are extensive, with bilateral involvements. Alternatively, deep cervical lymph nodes may be infected by tuberculosis that primarily invades the thoracic or abdominal lymph nodes and spreads via lymph vessels.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


