Adenomyomatosis: Mural GB wall thickening due to formation of intramural diverticula (Rokitansky-Aschoff sinuses) with smooth muscle and epithelial proliferation
Cholesterolosis: Deposition of foamy, cholesterol-laden histiocytes in subepithelium of GB
MR: High-signal cystic spaces (with curvilinear arrangement) on T2WI/MRCP within focally or diffusely thickened GB wall (string of beads or pearl necklace sign)
– Cystic nonenhancing spaces within thickened GB wall
• Cholesterolosis
US: Multiple small (< 10 mm) nonshadowing iso-/hyperechoic polyps with “comet tail” & twinkle artifact
MR: Small, round polyps with intermediate T1/T2 signal
CT: Usually imperceptible
CLINICAL ISSUES
• Virtually always asymptomatic, but may very rarely present with RUQ pain
• Almost always an incidental finding with no significance
Must be correctly differentiated from malignancy based on imaging appearance
Adenomyomatosis may rarely require cholecystectomy if symptomatic or if imaging findings are equivocal and there is concern for GB carcinoma
Cholesterol polyps may be resected when large or when growth is documented
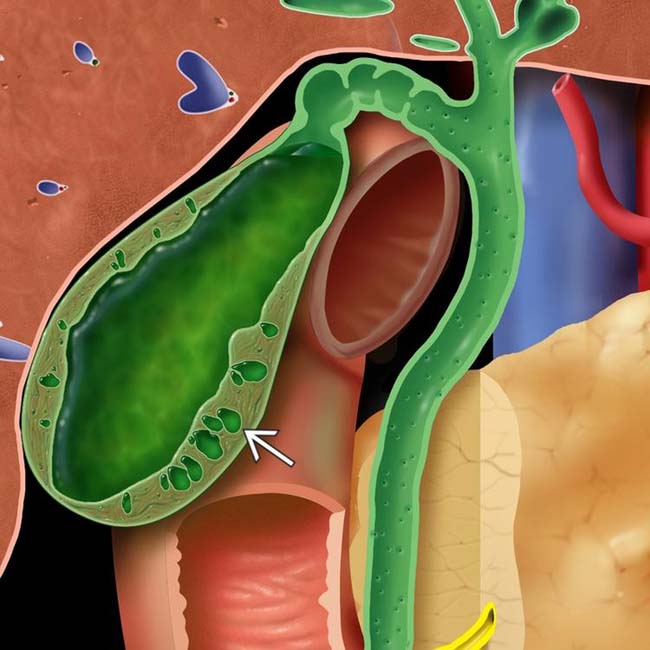
(Left) Schematic drawing of adenomyomatosis illustrates a thickened gallbladder (GB) wall with multiple intramural cystic spaces .
(Right) Ultrasound of an elderly woman with right upper quadrant pain shows tiny echogenic foci within the anterior wall of the GB and posterior “comet tail” artifacts . This appearance is likely caused by reverberation of the ultrasound pulse within cholesterol crystals in the GB subepithelium.
(Left) Ultrasound image demonstrates diffuse thickening of the GB wall with numerous foci of “comet tail” artifact , classic for adenomyomatosis. Note the presence of a gallstone , found in 90% of cases.
(Right) Color Doppler ultrasound demonstrates “twinkle” artifact associated with the echogenic reflectors within the thickened GB wall. “Comet tail” and twinkle artifacts are due to reverberation within cholesterol deposited within epithelial penetrations (Rokitansky-Aschoff sinuses).
• Idiopathic, nonneoplastic, and noninflammatory proliferative disorder that results in GB wall thickening
Subclassified into 2 entities
Adenomyomatosis
– Mural GB wall thickening due to exaggeration of normal luminal epithelial folds and formation of intramural diverticula (Rokitansky-Aschoff sinuses) in conjunction with smooth muscle and GB epithelial proliferation
Cholesterolosis
– Deposition of foamy, cholesterol-laden histiocytes in subepithelium of GB
– Numerous small accumulations (strawberry GB) or larger polypoid deposit (cholesterol polyp)
IMAGING
General Features
• Best diagnostic clue
Adenomyomatosis
– Focal (typically fundal) or diffuse GB wall thickening with intramural cystic spaces containing echogenic foci and “comet tail” artifacts
Cholesterolosis
– Echogenic GB polyps with associated “comet tail” artifact
• Location
Cholesterolosis: Superficial GB wall (epithelium)
Adenomyomatosis: Deep GB wall (muscular layer)
– Fundal (most common), segmental mid-body (“hourglass” configuration of GB), or diffuse
• Size
Cholesterol polyps typically 5-10 mm
CT Findings
• Adenomyomatosis
Segmental or diffuse GB wall thickening
– May present as fundal enhancing soft tissue nodule
Cystic nonenhancing spaces (Rokitansky-Aschoff sinuses) within thickened GB wall (usually within fundal mass)
– Cystic spaces most important feature to differentiate adenomyomatosis from GB carcinoma
– Ancillary findings favoring adenomyomatosis: Smooth borders without evidence of biliary ductal dilatation, hepatic invasion, or regional adenopathy
Often brisk wall enhancement post contrast
• Cholesterolosis: Subepithelial cholesterol and small cholesterol polyps usually imperceptible on CT
MR Findings
• Cholesterolosis
Small, round, intraluminal polyps juxtaposed against low T1WI signal and high T2WI signal bile
– Nodules are homogeneous and of intermediate signal intensity on both T1WI and T2WI
– Nodules are directly attached to GB wall
• Adenomyomatosis
T1-hypointense foci within thickened GB wall corresponding to bile-filled intramural diverticula
– Occasionally T1-hyperintense due to inspissated bile/debris within Rokitansky-Aschoff sinuses
T2WI/MRCP high signal cystic spaces (with a curvilinear arrangement) within focally or diffusely thickened GB wall (string of beads or pearl necklace sign)
Cystic spaces show no enhancement on T1WI C+ images
Diffusion weighted imaging (DWI) not a reliable means of distinguishing cancer from adenomyomatosis
• MR is highly accurate (> 90%) in differentiation of adenomyomatosis from GB carcinoma
Ultrasonographic Findings
• Grayscale ultrasound
Adenomyomatosis
– Focal, segmental, or diffuse wall thickening
Focal or localized form the most common, usually affecting GB fundus
Segmental form causes annular thickening of GB wall, resulting in strictures: Annular thickening in GB mid body results in “hourglass” appearance
Diffuse form results in wall thickening of entire GB
Only gold members can continue reading. Log In or Register to continue

 US: Focal, segmental, or diffuse wall thickening with anechoic intramural spaces, intramural echogenic foci ± acoustic shadowing, “comet tail” artifacts, & twinkle artifact
US: Focal, segmental, or diffuse wall thickening with anechoic intramural spaces, intramural echogenic foci ± acoustic shadowing, “comet tail” artifacts, & twinkle artifact MR: High-signal cystic spaces (with curvilinear arrangement) on T2WI/MRCP within focally or diffusely thickened GB wall (string of beads or pearl necklace sign)
MR: High-signal cystic spaces (with curvilinear arrangement) on T2WI/MRCP within focally or diffusely thickened GB wall (string of beads or pearl necklace sign)






 .
.
 within the anterior wall of the GB and posterior “comet tail” artifacts
within the anterior wall of the GB and posterior “comet tail” artifacts  . This appearance is likely caused by reverberation of the ultrasound pulse within cholesterol crystals in the GB subepithelium.
. This appearance is likely caused by reverberation of the ultrasound pulse within cholesterol crystals in the GB subepithelium.
 , classic for adenomyomatosis. Note the presence of a gallstone
, classic for adenomyomatosis. Note the presence of a gallstone  , found in 90% of cases.
, found in 90% of cases.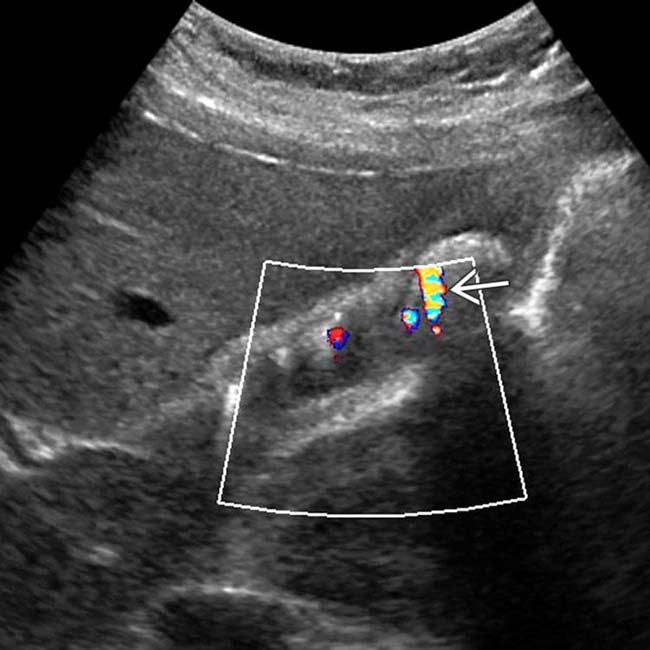
 associated with the echogenic reflectors within the thickened GB wall. “Comet tail” and twinkle artifacts are due to reverberation within cholesterol deposited within epithelial penetrations (Rokitansky-Aschoff sinuses).
associated with the echogenic reflectors within the thickened GB wall. “Comet tail” and twinkle artifacts are due to reverberation within cholesterol deposited within epithelial penetrations (Rokitansky-Aschoff sinuses).















 Adenomyomatosis
Adenomyomatosis Segmental form causes annular thickening of GB wall, resulting in strictures: Annular thickening in GB mid body results in “hourglass” appearance
Segmental form causes annular thickening of GB wall, resulting in strictures: Annular thickening in GB mid body results in “hourglass” appearance







