Fig. 1
Ophthalmic origin of the middle meningeal artery. Cerebral angiogram, lateral projection, early (a) and late arterial phase (b) of selective left internal carotid artery injection demonstrate reconstitution of the middle meningeal artery (white arrows) via the ophthalmic artery (black arrow) through the recurrent meningeal artery (black arrowhead). (c) Notice that the middle meningeal artery does not opacify on the selective external carotid artery injection. sta superficial temporal artery, ima internal maxillary artery
Multiple anastomoses between branches of the ECA and OA exist, and only the most clinically relevant variants will be described here. For a more detailed review, the articles by Hayreh [11] and Perrini et al. [5] are recommended. The recurrent meningeal artery is a critical anastomosis when attempting embolization of convexity meningiomas. It typically projects posteriorly to the OA through the superior orbital fissure.
Another important group of anastomoses is between the anterior and posterior ethmoidal branches of the OA and the distal branches of the internal maxillary artery, namely, the sphenopalatine and greater palatine arteries (Fig. 2). The presence of such anastomoses should be explored on cerebral angiography when planning embolization for epistaxis [12].
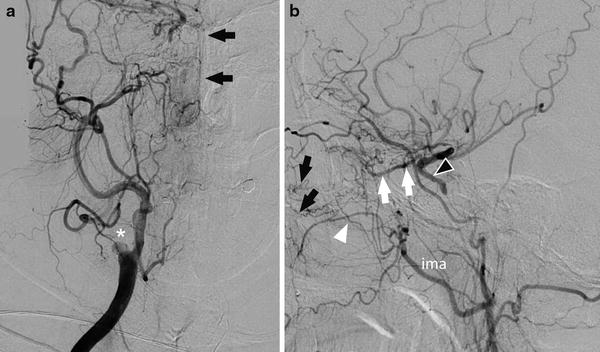
Fig. 2
Ophthalmic artery–internal maxillary artery anastomoses. Cerebral angiogram in a patient with chronic right internal carotid artery occlusion (asterisk on anteroposterior [AP] view), AP (a) and lateral (b) views, shows reconstitution of the ophthalmic artery (white arrows) through the anterior and posterior ethmoidal branches (black arrows point to the nasal blush at the site of anastomoses within the nasal cavity). White arrowhead – infraorbital artery of the internal maxillary artery. Black arrowhead – cavernous internal carotid artery; ima internal maxillary artery
Additional examples of potential anastomoses involving the OA include the superficial temporal artery branches such as the zygomatico-orbital artery, terminal nasal branches of the facial artery, and the infraorbital branch of the internal maxillary artery (Fig. 3). Extracranial–intracranial anastomoses have been described between the MMA, superficial temporal artery, occipital artery, and the cortical leptomeningeal arteries [13] (Fig. 4).
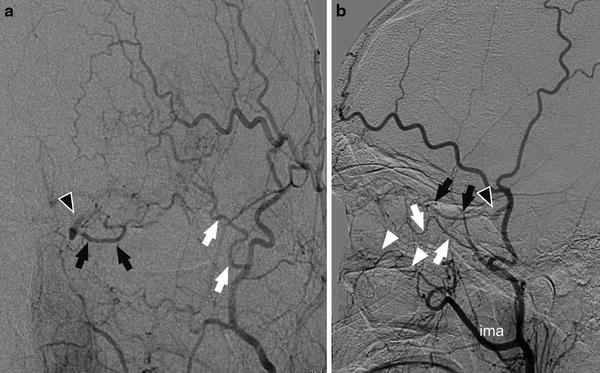
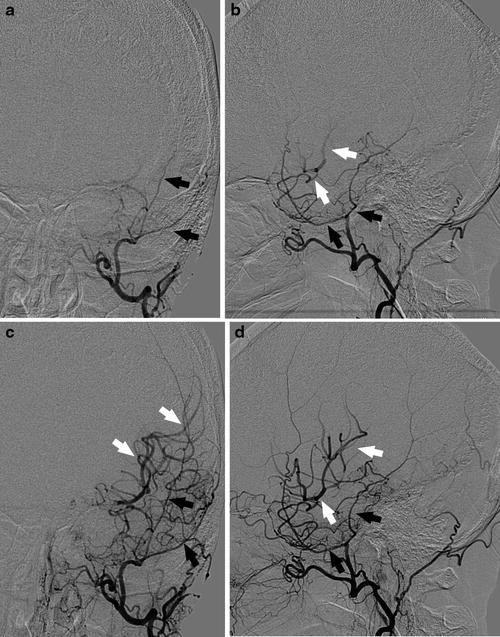
Fig. 3
Superficial temporal artery anastomoses to the ophthalmic artery. Cerebral angiogram, AP (a) and lateral (b) views, shows opacification of the ophthalmic artery (black arrows) and the supraclinoid internal carotid artery (black arrowheads) via the zygomatico-orbital branch (white arrow) of the superficial temporal artery. Another anastomosis involves the infraorbital branch (white arrowheads) of the internal maxillary artery (ima)
Fig. 4
Cortical leptomeningeal anastomoses. Cerebral angiogram, early arterial intracranial AP (a) and lateral (b) views and late arterial intracranial AP (c) and lateral (d) views, shows cortical leptomeningeal anastomoses between the middle meningeal artery (black arrows) and the middle cerebral artery (white arrows)
Internal Carotid Artery Anastomoses
Important anastomoses within the petrocavernous segment of the ICA are described below. They can often be identified on cerebral angiograms in cases of cervical ICA occlusion and are a critical component of dural arteriovenous malformations in this region.
The inferolateral trunk is a remnant of the dorsal OA and consists of several branches that provide supply to the cranial nerves and the gasserian ganglion. Anteroinferiorly, a characteristic serpentine-like anastomosis with the maxillary artery through the artery of the foramen rotundum can be observed (Fig. 5). Other anastomoses include the recurrent artery of foramen lacerum (which connects with the ascending pharyngeal artery), branches of the MMA (seen laterally through the foramen spinosum), branches of the accessory meningeal artery (seen posteriorly), and branches of the ascending pharyngeal artery (carotid branch of the superior pharyngeal branch through the foramen lacerum) (Fig. 6).
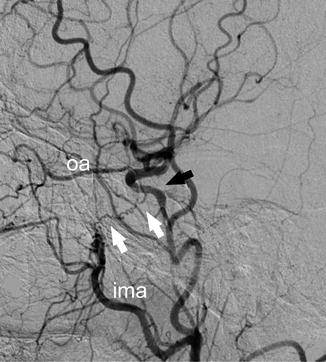
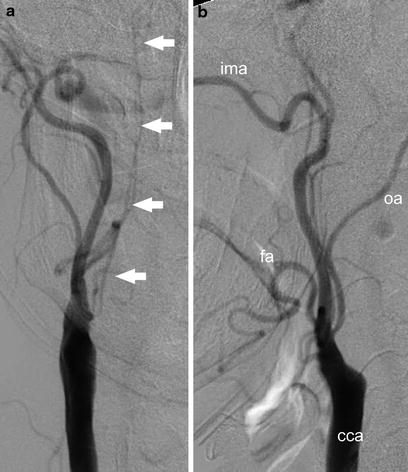
Fig. 5
Artery of foramen rotundum. Cerebral angiogram, AP view, demonstrates a characteristic serpentine-like artery of foramen rotundum (white arrows) directed at the base of the sella, which is an anastomosis between the internal maxillary artery (ima) and the cavernous segment of the internal carotid artery (black arrow). oa ophthalmic artery
Fig. 6
Ascending pharyngeal artery anastomosis. Cerebral angiogram, AP (a) and lateral (b) views, shows a typical appearance of the ascending pharyngeal artery. The superior pharyngeal branch of the pharyngeal trunk (white arrows) gives off the carotid branch, which creates an anastomosis with the inferolateral trunk (not shown). cca common carotid artery, fa facial artery, ima internal maxillary artery, oa occipital artery
A rare finding on cerebral angiography is hypertrophy of the vasa vasorum after complete occlusion of the cervical ICA [14] (Fig. 7). Extensive proliferation of the vasa vasorum can lead to anterograde recanalization of the ICA distally, such as at the level of the petrocavernous segment, and can be confused with anastomoses originating from the ascending pharyngeal artery. Visualization of tortuous vascular channels that project over the expected course of the cervical ICA rather than the ascending pharyngeal artery helps in differentiating the two conditions. The ascending pharyngeal artery typically originates from the posterior wall of the ECA trunk, although rarely its origin can be seen from the proximal cervical ICA.
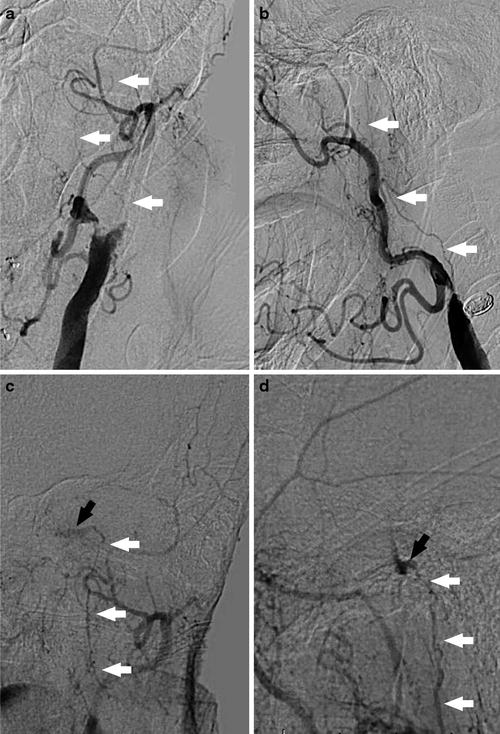
Fig. 7
Vasa vasorum of the internal carotid artery. Cerebral angiogram, cervical AP (a) and lateral (b) views and cranial AP (c) and lateral (d) views in a case of chronic cervical left internal carotid artery occlusion. The petrous segment of the internal carotid artery (black arrows) reconstitutes via a prominent network of vasa vasorum, which appear as tortuous channels following the expected course of the cervical internal carotid artery (white arrows)
The meningohypophyseal trunk of the ICA supplies the pituitary gland, the clival region, and the meninges of the tentorium. Through its tentorial branches, which are seen more anteriorly, it can form anastomoses with petrous branches of the MMA. Another common anastomosis of the meningohypophyseal trunk involves its lateral clival artery and neuromeningeal branches of the ascending pharyngeal artery.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


