Various modalities, including computed tomography (CT), MR imaging, and PET/CT, are used in the radiological assessment of the treated orbit. Understanding the different surgical procedures used for orbital and ocular adnexal tumors and the imaging characteristics of recurrent tumors after complex reconstructive procedures in the orbital region is critical. Knowledge of treatment complications, including infection, osteoradionecrosis, radiation necrosis, radiation-associated secondary sarcomas, and tumor recurrence, is also important. To assist the radiologist, this article highlights several common orbital surgical procedures and complications that may arise following treatment.
Key points
-
•
Treatment of orbital tumors and diseases affecting the orbit requires a multidisciplinary approach, both before and after treatment.
-
•
Radiology plays a crucial role in evaluating the orbital area after these treatments.
-
•
This article discusses the imaging appearance of the orbit following treatment of tumors and cancer-related conditions, including complex reconstructive procedures and adjuvant therapy.
-
•
It also addresses potential complications such as infection, osteoradionecrosis, radiation necrosis, radiation-associated secondary tumors, and tumor recurrence.
Abbreviations
| FDG | 18 F-2-deoxy- d -glucose |
| GDD | glaucoma drainage devices |
| PA | pleomorphic adenoma |
| RION | radiation-induced optic neuropathy |
Introduction
Treatment of orbital lesions is often multidisciplinary and involves a combination of surgery, chemotherapy, radiation, and immunotherapy. Radiologists may find it difficult to interpret images after treatment due to the changes in the anatomy caused by these therapies. To address this, it is essential to understand the original tumor characteristics, the timing and type of treatments, and the patient’s clinical status at the time of the examination. Surgery may involve removing a part of the globe or the entire globe, various parts of the orbital structures or the entire orbital content, followed by reconstruction using various types of flaps. A prosthesis might be inserted after surgery for cosmetic reasons. Chemotherapy and radiation can cause tissue damage, including in the treatment area, which can affect the brain, bone, and soft tissues. Despite treatment, tumors can recur or develop related to the treatment, and it is important to distinguish these from normal posttreatment changes. This article discusses common treatments for orbital and ocular adnexal lesions and their typical imaging features in an attempt to aid radiologists in their interpretation of these studies.
Imaging Approach to the Treated Orbit
Plain radiographs can screen patients with suspected foreign bodies or metallic implants before an MR imaging, but are rarely used otherwise. CT is performed with thin axial slices that can be reconstructed in the coronal and sagittal planes or reformatted in any plane deemed necessary. The images are displayed with soft tissue and bone algorithms. CT is generally superior for evaluating bony structures for signs of remodeling, destruction, or fractures caused by trauma, tumors, or treatment effects. MR imaging offers better soft tissue delineation without exposing patients to ionizing radiation, which is especially important for pediatric patients. Fat-suppression techniques with T2 and T1 postcontrast sequences aid in better delineating lesions. Diffusion-weighted sequences can assist in monitoring treatment response and detecting tumor recurrences. CT and MR angiography may be used to assess orbital, intracranial, and neck vascularity and are useful in managing complications from various treatments. PET/CT using 18 F-2-deoxy- d -glucose (FDG) is used not only for staging ophthalmic tumors, particularly for detecting distant metastases and monitoring treatment response, but also aids in the detection of local recurrences. For a more detailed description, the reader is referred to the article Orbital imaging modalities and recent updates by Dr. Sooyoung Martin.
Imaging of the Eye (Globe)
Article- Imaging of the Globe: Anatomy and Pathology by Dr. Liang Tan and Dr. Hallinan, covers postoperative changes to the globe, including retinal detachment, glaucoma drainage devices (GDD), lens replacements, scleral buckling, silicone oil tamponade, pneumatic retinopexy, and orbital prostheses.
Imaging Findings after Evisceration and Enucleation
Removal of the globe may be necessary for various reasons, including malignancies like retinoblastoma and melanoma. Evisceration refers to the surgical removal of the contents of the globe, including the cornea (the clear portion of the globe covering the iris and pupil). The sclera, adnexal soft tissues (eyelid, conjunctiva, and lacrimal gland), and the extraocular muscles remain intact ( Fig. 1 ). Another common reason for evisceration includes removing a painful blind eye caused by various conditions, such as chronic glaucoma, retinal ischemia, ocular trauma, and infection. An orbital implant is inserted into the scleral shell that is still attached to the extraocular muscles after evisceration. An ocular shell prosthesis is placed for cosmesis.
Evisceration. A 65-year-old female with conjunctival squamous cell carcinoma treated with evisceration. ( A ) Sagittal T1 postcontrast MR imaging shows an enhancing lesion in the inferior conjunctiva with extension under the globe ( arrow ). ( B , C ) Axial T1 postcontrast and axial T2 MR images show the appearance of the residual sclera after evisceration ( small arrows ) and a scleral prosthesis ( large arrows ).
Enucleation of a globe is an end-stage procedure for the treatment of a variety of ocular diseases. An enucleation removes the globe from its connections to the orbit, including the optic nerve and the extraocular muscles, with the remaining connections staying in place ( Fig. 2 ). At the time of enucleation, an orbital implant is typically placed in the socket, and usually the extraocular muscles are attached to the anterior surface of the orbital implant. An ocular prosthesis is placed for cosmesis. Indications for an enucleation include trauma, intraocular tumors such as retinoblastoma and uveal melanoma, end-stage glaucoma, and infection (endophthalmitis). , For malignant intraocular tumors such as retinoblastoma and melanoma, enucleation is the appropriate surgical procedure. ,,
Enucleation. A 46-year-old female with left uveal melanoma treated with enucleation and radiation. ( A ) Axial T1 postcontrast MR imaging orbits shows an enhancing uveal lesion in the left globe ( arrow ). ( B , C ) Axial T1 postcontrast and axial T2 MR images show the appearance of the orbit after enucleation and placement of an orbital implant ( small arrows ) and ocular prosthesis ( large arrows ).
With endophthalmitis as the indication for an enucleation, an infection may occur after surgery and can appear as an abnormal fluid collection, fat stranding, enhancement, and gas in the enucleation cavity. Similarly, an infected fluid collection can form around a prosthesis or implant.
Orbital Exenteration
Orbital tumors may require treatment with a combination of surgery, including orbital exenteration, chemotherapy, and radiation. An exenteration might be necessary depending on the tumor’s location and extent. It involves removing the contents of the orbit, such as the globe, optic nerve, extraocular muscles, and parts of the surrounding bony structures ( Figs. 3 and 4 ). The goal of an exenteration is to excise the tumor with free margins. Malignancies that are most often treated with an exenteration include lacrimal gland adenoid cystic carcinoma, conjunctival and uveal melanoma, or locally advanced basal cell carcinoma, squamous cell carcinoma, and sebaceous carcinoma. The overall exenteration rate is decreasing with the advancement in neoadjuvant therapies. Life-threatening orbital infections may also require an exenteration. Following an exenteration, a flap reconstruction may be performed. Residual optic nerve and extraocular muscles may remain in the orbital apex and should not be mistaken for a tumor. Over time, these residual structures can atrophy. Lesions extending to adjacent structures outside the orbit may require a maxillectomy, skull base resection, craniofacial resection, and reconstruction of the defect. ,
Exenteration with fasciocutaneous flap reconstruction. A 66-year-old woman with a history of multiple recurrent conjunctival melanomas, with a recurrence in the right upper eyelid. ( A ) Axial T1 postcontrast MR imaging orbits shows an enhancing lesion in the right upper eyelid ( arrow ). ( B , C ) Axial T1 postcontrast and axial T2 MR images show the appearance of the orbit after exenteration and fasciocutaneous flap reconstruction ( arrows ).
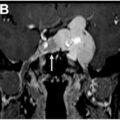
Exenteration with myocutaneous flap reconstruction. A 69-year-old man with a right lacrimal gland adenoid cystic carcinoma who underwent orbital exenteration with myocutaneous flap reconstruction. ( A ) Axial T1 postcontrast MR imaging orbits shows an infiltrative right orbital mass ( arrows ). ( B ) Axial T1 noncontrast MR imaging shows the fat ( large arrow ) and muscular components of the myocutaneous flap with a striated appearance ( small arrow ). ( C ) Axial T2 MR imaging with fat saturation shows a hypointense appearance of the fat component (large arrow ) and a hyperintense appearance of the muscular component ( small arrow ). ( D ) Axial T1 postcontrast MR imaging with fat saturation shows a hypointense appearance of the fat component ( large arrow ) and an isointense appearance of the muscular component ( small arrow ).
When evaluating the orbit after the globe is surgically removed, it is important not to confuse any remaining orbital structures, such as the optic nerve and extraocular muscles, with residual or recurrent tumor. Sometimes, this requires short-term follow-up, as these remaining structures may appear swollen in the immediate postoperative period, which will resolve ( Fig. 5 ). Additionally, atrophy of the optic nerve remnant and the optic chiasm can develop over time.
Postoperative change following exenteration. A 69-year-old man with a right lacrimal gland adenoid cystic carcinoma who underwent orbital exenteration with myocutaneous flap reconstruction. ( A , B ) Axial and coronal T1 postcontrast MR imaging orbits show enhancement in the right orbital socket ( large arrows ) surrounding the residual optic nerve ( small arrows ). ( C ) Axial 18 F-FDG-PET/CT shows mild uptake in the right orbital socket with an SUV measuring 3.8 ( arrow ). ( D , E ) Axial and coronal T1 postcontrast MR imaging orbits show decreasing enhancement in the right orbital socket that involved the residual extraocular muscles ( arrows ) on follow-up. ( F ) Axial 18 F-FDG-PET/CT shows resolution of uptake in the right orbital socket after 2 months.
Fasciocutaneous and Myocutaneous Flap Reconstruction
Following an orbital exenteration, various grafts and flaps can be used to reconstruct the defect. Fasciocutaneous flaps consist of skin and subcutaneous soft tissue that includes fascia and fat (see Fig. 3 ), while myocutaneous flaps include skin, subcutaneous soft tissue, and muscle ( Fig. 4 ). ,, If an orbital prosthesis is planned, a skin graft or fasciocutaneous flap is used, creating an open cavity that can accommodate a prosthesis. A myocutaneous flap results in a closed cavity as muscular soft tissue fills the cavity. After an extended surgery that exposes adjacent areas such as the orbital roof, paranasal sinuses, the dura in the intracranial compartment, and/or infratemporal fossa, a vascularized free flap can be placed to reconstruct the defect. Often, a vascularized free flap is placed to cover the orbital defect after exenteration, especially if radiation therapy is planned for the treatment of the underlying malignancy. ,,,
On MR imaging, the fat component within fasciocutaneous and myocutaneous flaps appears T1 hyperintense, while other tissues, including the muscular part of a myocutaneous flap, are T2 isointense to hyperintense (see Figs. 3 and 4). A striated appearance is present in the muscular component of a myocutaneous flap (see Fig. 4 ). Homogeneous or heterogeneous enhancement within the flaps may be observed, and enhancement of the flap and edema should not be mistaken for recurrent tumor. Over time, these features may remain stable or decrease. The flaps can also retract over time, with a corresponding decrease in volume. An increase in T2 signal and enhancement may occur after a flap is irradiated, but these changes tend to diminish over time ( Fig. 6 ).
Radiation effects on myocutaneous flap. (Same patient as Fig. 4 ). ( A , B ) Axial T1 postcontrast and axial T2 MR imaging of the orbits show the appearance of the myocutaneous flap after surgery. ( C ) Axial T1 postcontrast MR imaging with fat saturation shows mild heterogeneous enhancement of the muscular component after radiation ( arrow ) that should not be confused for tumor. ( D ) Axial T2 MR imaging with fat saturation shows a persistent hyperintense appearance of the muscular component after radiation ( arrow ).
Over 20% of exenterations performed for tumor resection involve posttreatment complications, including infection ( Figs. 7 and 8 ), flap necrosis, fistula formation ( Fig. 9 ), hemorrhage ( Fig. 10 ), and cerebrospinal fluid (CSF) leak. , Fistulas can extend into the ethmoid air cells and other sites, appearing as air-filled channels on CT.
Abscess. A 63-year-old man with left nasal cavity squamous cell carcinoma underwent suprastructure maxillectomy with orbital exenteration and myocutaneous flap reconstruction, who developed an abscess in the orbital socket. ( A ) Coronal T1 postcontrast MR imaging shows an enhancing left maxillary sinus mass with extension through the orbital floor into the inferior orbit ( arrows ). ( B ) Coronal T1 postcontrast MR imaging shows a peripherally enhancing fluid collection in the superonasal left orbit ( large arrow ) adjacent to the flap ( small arrow ). ( C ) Axial diffusion-weighted image (DWI) shows signal hyperintensity in the fluid collection ( arrow ). ( D ) Axial apparent diffusion coefficient map shows signal hypointensity in the collection, confirming restricted diffusion in the abscess ( arrow ).
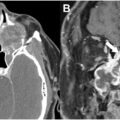
Abscess. A 71-year-old man with a sinonasal undifferentiated carcinoma (SNUC) involving the orbit and a complex treatment history including multiple surgeries, including orbital exenteration and flap reconstruction, chemotherapy, and radiation, who developed osteoradionecrosis and an abscess at the operative site. ( A ) Coronal T1 postcontrast MR imaging shows an SNUC in the left infratemporal fossa that extends into the inferotemporal left orbit ( arrows ). ( B ) Coronal T1 postcontrast MR imaging shows a large myocutaneous flap in the left face, infratemporal fossa, and orbit ( arrows ). ( C ) Photograph showing swelling and induration of the left face related to an underlying infection. ( D ) Coronal T1 postcontrast MR imaging shows a peripherally enhancing fluid collection consistent with an abscess along the deep margin of the flap ( large white arrow ) and enhancement in the flap related to the infection ( small white arrow ). Note the enhancing radiation necrosis in the left temporal lobe ( black arrow ).
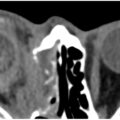
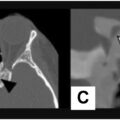
Fistula. A 69-year-old man with right eyelid squamous cell carcinoma who underwent orbital exenteration and myocutaneous flap reconstruction. After several revision surgeries of the flap, he developed a nasal cutaneous fistula. ( A ) Axial T1 postcontrast MR imaging shows a tumor in the right eyelid, extraconal orbit, and temporal scalp soft tissues ( arrows ). ( B ) Coronal T1 postcontrast MR imaging shows the myocutaneous flap in the right orbit and face ( arrows ). ( C , D ) Sagittal and coronal CT, bone window, shows complex postoperative changes with multiple fistulas extending from the operative site to the face and ethmoid air cells ( arrows ).
Hemorrhage. A 33-year-old male with invasive poorly differentiated squamous cell carcinoma of the right medial canthus, nasolacrimal duct, orbit, and paranasal sinuses was treated with exenteration and presented with blood draining from the operative site. Axial CT with contrast shows a hyperdense hemorrhage within the flap ( arrow ).
Orbital Implants and Ocular Prosthesis after Enucleation/Evisceration
After the globe is eviscerated or enucleated, various implants may be used to restore volume to the orbital socket and improve its appearance (see Figs. 1, 2 and 11 ). A porous implant contains holes similar to bone trabeculae, allowing for the ingrowth of vascular connective tissue. This ingrowth decreases the risk of implant extrusion, improves movement, and lowers infection risk. Other implants are smooth, nonporous, and made of glass, silicone, and polymethyl methacrylate. These orbital implants come in different appearances and should not be mistaken for foreign bodies, bone, or phthisis bulbi (a shrunken and disorganized globe). On follow-up imaging, any implant extrusion or infection should be reported.
Recurrent tumor and reconstruction. A child with bilateral retinoblastoma who underwent bilateral enucleation later developed a recurrence in the right orbit and intracranial compartment and underwent surgical resection with mesh reconstruction. ( A ) Axial T1 postcontrast MR imaging shows retinoblastoma in bilateral globes ( arrows ). ( B ) Axial CT, bone window, shows bilateral orbital implants ( arrows ). ( C ) Axial T1 postcontrast MR imaging shows recurrent tumor in the right orbit and temporal lobe ( arrows ). ( D ) Axial T1 postcontrast MR imaging shows postoperative changes after recurrent tumor resection, titanium mesh reconstruction ( small arrows ), and ocular prosthesis placement ( large arrow ). ( E , F ) Coronal and sagittal CT, bone windows, show the titanium mesh reconstruction (small arrows ) and an orbital implant ( large arrows ).
Orbital Wall Reconstruction
If extensive orbital surgery involves resection of the orbital wall or floor, reconstruction may be performed to restore the bony structures, orbital contour and volume, minimize enophthalmos, and improve cosmesis ( Figs. 11 and 12 ). , The repair of the orbital wall can be done using bone flaps, autologous cartilage, titanium mesh, silicone sheet implants, and metallic plates. ,, When assessing the postoperative orbit after complex reconstruction, it is important to observe the positioning of implants, such as bone flaps and titanium mesh, as well as any movement over time and impingement of ocular structures, such as the extraocular muscles, by the implant.
Orbital reconstruction. A 55-year-old man with a left maxillary sinus tumor that extended into the inferior left orbit who underwent a left maxillectomy and free fibula flap reconstruction and placement of a Computer-Aided Design and Computer-Aided Manufacturing (CADCAM) orbital floor plate. He developed osteoradionecrosis and recurrent infections following postoperative radiation therapy and subsequently underwent scapula bone flap reconstruction. ( A ) Coronal T1 postcontrast MR imaging shows a left maxillary sinus tumor with involvement of the orbital floor and inferior orbit ( arrows ). ( B , C ) Coronal and axial CT, bone windows, show the fibular free flap ( large arrow ) and the CADCAM prosthesis ( small arrows ).
Radiation Effects
Side effects from radiation therapy used to treat orbital tumors can appear on imaging during both early and late posttreatment periods and may be seen within or outside the orbit. These effects include orbital fat atrophy, optic neuropathy, vasculopathy, central nervous system (CNS) radiation necrosis, and osteoradionecrosis. Radiation-associated atrophy of orbital fat can lead to enophthalmos and decreased ocular motility. Contraction of the orbital contents, including the extraocular muscles, can also contribute to these symptoms and imaging can evaluate the reduction in orbital volume.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


