This article provides an imaging-focused overview of conditions affecting vision that localize to the central skull base. Both neoplastic and nonneoplastic processes may arise from the sphenoid bone, sella turcica, and adjacent structures, with potential involvement of critical neurovascular pathways. Because clinical presentations in this region often overlap, identifying distinguishing features on computed tomography and MR imaging is essential for accurate diagnosis. The discussion highlights key imaging findings of pathology affecting visual function arising within and around the central skull base.
Key points
-
•
Skull base pathology is a relatively common cause of visual disturbance.
-
•
Clinical manifestations of disease in this region typically include headache, compressive optic neuropathy, and/or ophthalmoplegia.
-
•
Careful evaluation of findings on computed tomography and MR imaging is imperative for localizing the lesion and generating an accurate differential diagnosis.
-
•
Important first steps in imaging evaluation are determining if the lesion arises directly from bone or external to the osseous structures.
-
•
Radiologists should be facile at describing anatomic structures affected by lesions in this region, particularly skull base foramina transmitting important neurovascular structures.
Abbreviations
| ADC | apparent diffusion constant |
| CT | computed tomography |
| DLBCL | diffuse large B-cell lymphoma |
| DWI | diffusion-weighted imaging |
| FD | fibrous dysplasia |
| PPF | pterygopalatine fossa |
| SOF | superior orbital fissure |
| STIR | short tau inversion recovery |
Introduction
Vision depends not only on the optic nerves but also on the complex anatomy of the central skull base and sellar/parasellar regions. This area represents a critical crossroads between the intracranial compartment, orbits, deep face, and suprahyoid neck, and is among the most anatomically intricate regions encountered in neuroimaging. Although visual symptoms often raise concern for primary optic nerve disease, numerous pathologies arising within or extending into the skull base can affect the visual pathways. Lesions may originate intracranially, from the skull base itself, or from adjacent extracranial compartments, and encompass a broad spectrum of neoplastic, infectious, inflammatory, developmental, and vascular processes. High-resolution, multiplanar computed tomography (CT) and MR imaging enable detailed assessment of this region, and a strong understanding of its anatomy is essential for accurate lesion localization, determination of site of origin, and development of a clinically meaningful, anatomy-based differential diagnosis for vision-related symptoms.
Normal anatomy of the optic nerve and sella
Orbital Apex
The orbital apex is intimately related to the central skull base, primarily through the lesser and greater wings of the sphenoid bone, which form substantial portions of the superior and lateral orbital walls. It functions as a key anatomic crossroads between the orbit, cavernous sinus, and central skull base via the optic canal and superior orbital fissure (SOF). Orbital processes may also extend posteriorly and inferiorly through the inferior orbital fissure into the pterygopalatine fossa (PPF), providing another route of skull base communication.
Optic Canal and Sphenoid Anatomy
The optic canal is a short but critical bony conduit within the lesser wing of the sphenoid that transmits the optic nerve and ophthalmic artery from the orbit into the middle cranial fossa. Its medial wall is formed by the anterolateral surface of the sphenoid body. The roof consists of a thin bony bridge known as the superior root of the lesser wing, while the lateral wall is formed by the optic strut (the inferior root of the lesser wing) and the anterior clinoid process.
The optic strut is a key landmark at the central skull base, separating the optic canal from the medial margin of the SOF. Just lateral to this, the SOF forms an oblique cleft between the greater and lesser sphenoid wings. Its medial portion lies directly anterior to the cavernous sinus, underscoring how orbital pathology can readily extend to parasellar structures. Inferiorly, the inferior orbital fissure is an oblique gap between the lateral orbital wall and floor. It communicates posteriorly with the PPF and laterally with the infratemporal fossa, providing an additional pathway between orbital and deep skull base spaces.
Transition from Orbit to Central Skull Base
Posterior to the optic canal, the prechiasmatic (cisternal) intracranial segment of the optic nerve enters the subarachnoid space of the central skull base. Here, it courses within the suprasellar cistern, just superior to the bony sella turcica, before converging with the contralateral nerve to form the optic chiasm. This region represents the direct anatomic transition from orbital structures to the sellar and parasellar compartments of the central skull base.
The sellar and suprasellar region includes the pituitary gland (anterior and posterior lobes), the pituitary infundibulum, and portions of the hypothalamus. The anterior pituitary (adenohypophysis) arises embryologically from Rathke’s pouch, whereas the posterior pituitary (neurohypophysis) develops as a downward extension of the hypothalamus. Because the optic chiasm rests immediately superior to the diaphragma sellae, sellar and suprasellar masses commonly produce visual symptoms as a result of compression of the chiasm.
Surrounding this region are critical neurovascular structures embedded within the central skull base. The intracranial segments of the internal carotid arteries course from the foramen lacerum to their termini adjacent to the optic chiasm. The paired cavernous sinuses lie along the lateral aspects of the sella turcica. Within their lateral walls and lumen pass cranial nerves III, IV, V1, V2, and VI, which then travel anteriorly through the SOF into the orbit—again highlighting the tight anatomic continuity between the orbit and parasellar skull base.
Clinical presentation
Headache and visual disturbance are common presentations for pathology affecting the orbit and parasellar skull base, often attributed to mass effect upon surrounding structures, and thus, a myriad of pathology can present with similar symptoms. Clinical symptoms of compressive optic neuropathy including visual field loss, loss of color perception, and decreased visual acuity typically occur over a protracted period. Regardless of underlying etiology, natural progression of compressive optic neuropathy can be devastating, beginning with subtle visual deficits and progressing to blindness if left untreated. , Diplopia attributable to ophthalmoplegia from compression or direct involvement of cranial nerves responsible for innervation of the extraocular muscles is a common presentation of pathology in this region and thus will be a recurring theme in this article.
Imaging Technique/Protocols
Of notable importance, direct endoscopy through the paranasal sinuses and/or clinical examination is often insufficient for evaluating lesions of the central skull base. Therefore, radiologists play an important role in diagnosis of these lesions. As with much pathology in the head and neck, CT and MR are complementary when generating an accurate differential diagnosis of pathology arising from central skull base. CT is often useful for describing aggressive features of a lesion or process such as erosive and destructive change, which may lead one away from considering benign or developmental pathology. On the other hand, MR imaging is necessary for evaluating signal and enhancement characteristics, and the relationship with the optic nerves in the setting of visual disturbances.
Imaging technique is usually tailored to the specific location being imaged. Most commonly thin cut CT images are included (sub 1 mm slices) in soft tissue and bone kernel. Dedicated MR imaging of the orbits with and without contrast is typically performed if there is concern for visual disturbance. Coronal short tau inversion recovery (STIR) is necessary to evaluate caliber and T2 signal abnormalities of the nerve. Importantly, coronal and axial T1-weighted imaging prior to contrast administration are imperative for evaluating soft tissue structures, such as the extraocular muscles. Coronal and axial T1-weighted postcontrast sequences with fat saturation are necessary to evaluate for pathologic enhancement. Additional sequences such as diffusion-weighted imaging (DWI) can be complementary and newer perfusion techniques may continue to improve diagnostic specificity. With these building blocks in mind, this study will begin with an overview of neoplastic abnormalities arising from the osseous structures that make up the skull base.
Neoplasm arising from bone
Neoplastic pathology within the skull base is an important cause of visual disturbance. In this article, we will cover malignancies both primary to the bone and arising elsewhere within the central skull base. For the practicing radiologist, a key diagnostic triage point is in determining whether the lesion originates from the bone itself. This review of malignancy will not be comprehensive, with less common conditions such as Ewing’s sarcoma and postradiation osteosarcomas of the skull base found in excellent reviews elsewhere.
Chordoma
Chordomas are malignant tumors arising from notochord remnants along the midline axial skeleton, and can arise cranially from the clivus or caudally from the sacrum. Approximately 30% to 40% of all chordomas arise from the central skull base or clivus. A spectrum of chordoma exists, from slow-growing, low-grade tumors to dedifferentiated tumors, and many of these tumors are locally invasive and highly recurrent. Patients with chordomas in the skull base tend to present earlier than those with lesions in the vertebral bodies or sacrum likely owing to the small, vulnerable neurovascular anatomy in this region.
Visual manifestations of these lesions are directly related to the rate and direction of growth of the tumor. More than half of patients experience ocular symptoms with diplopia being most common, followed by intermittent diplopia, and reduced visual acuity. Ophthalmoplegia resulting in diplopia can most commonly be attributed to the lesions impact on cranial nerve VI (abducens nerve) usually within the cisternal segment or along the course of Dorello’s canal as it traverses the clivus. However, other cranial nerves are often involved, including III, IV, and VI. Importantly, the cranial growth of these lesions within and along the posterior margin of the clivus can also result in compression of the optic chiasm leading to compressive pathology such as visual field defects, papilledema, and in the later stages, optic atrophy.
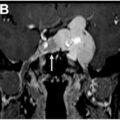
Chordomas usually appear as lytic lesions on CT centered within the skull base or clivus. They classically demonstrate the “thumbprint sign,” or extension posteriorly into the prepontine cistern with impression upon the pons ( Fig. 1 ). There are often internal areas of calcification. MR of the lesion classically demonstrates hyperintense signal on T2-weighted images with mild enhancement following administration of contrast. It typically exhibits relatively lower apparent diffusion constant (ADC) values on DWI than chondrosarcoma.
Chordoma. Axial T2-weighted MR images at the level of Meckel’s caves demonstrate a lobulated T2 hyperintense mass originating from a midline location within the clivus ( A, solid black arrow ) and extending into the prepontine cistern, “thumbprint sign” ( B, solid white arrow ). Precontrast ( C ) and postcontrast ( D ) administration T1-weighted images at the same level demonstrate solid enhancement.
Chondrosarcoma
Chondrosarcomas are often thought of as the off-midline relative of the chordoma, owing to the similar imaging manifestations and clinical presentation. These lesions are slow growing, found in the appendicular skeleton, and arise from cartilaginous tissue. Specifically, the cartilaginous tissue of the petroclival fissure is the classic, off-midline location where these tumors commonly originate. Patients usually present with headache and other symptoms related to neurovascular compression, as with many lesions in this location.
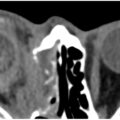
Imaging characteristics typically demonstrate a lobulated, off midline mass arising from the petroclival fissure with destructive osseous features and soft tissue components. These lesions also characteristically exhibit internal chondroid matrix, or ring-and-arc formation ( Fig. 2 ). MR features include heterogeneous, mild enhancement on T1-weighted images following contrast administration. A classic feature of skull base chondrosarcoma is the presence of hyperintense signal on T2-weighted images related to chondroid matrix and water content. In contradistinction to the chordoma, these often have less true reduced diffusivity and can be distinguished from other lesions in this region by their relative hypovascularity ( Fig. 3 ).
Chondrosarcoma. Sagittal ( A ) and axial ( C ) CT images of the skull base demonstrate a destructive lesion arising from within the sphenoid with internal rings and arcs ( solid white arrow ) . There is marked hyperintense signal on T2-weighted sagittal MR sequences ( B ) with axial precontrast T1-weighted sequences ( D ) and postcontrast sequences ( E ) demonstrating heterogeneous internal contrast enhancement.
Chondrosarcoma. Axial CT images ( A ) demonstrate a destructive process along the left petroclival fissure ( solid white arrow ) . Axial DWI sequences ( B ) demonstrate mild reduced diffusivity within the lesion ( dashed arrow ). T2-weighted images ( C ) demonstrate T2 hyperintense signal within the lesion ( black arrowhead ) . Precontrast ( D ) and postcontrast ( E ) T1-weighted images demonstrate only mild internal enhancement ( white arrowheads ) .
Plasmacytoma
Solitary plasmacytomas of the skull base are a rare pathology that can present with visual abnormalities. In the absence of systemic plasma cell dyscrasia, a solitary plasmacytoma is defined by monoclonal plasma cells isolated to a specific site and is uncommon, reportedly accounting for less than 10% of plasma cell neoplasms. Most commonly these lesions occur within vertebrae, though they can present as solitary skull base lesions, calvarial lesions or extramedullary lesions within the nasal cavity. Clinical presentation is most commonly related to mass effect upon neurovascular structures, as with much pathology of the skull base. Headaches, diplopia, and visual field deficits are frequent with the abducens nerve being the most commonly affected.
While histologic confirmation is necessary for diagnosis, imaging often helps direct the clinical team toward a correct diagnosis. Of particular importance is identifying whether the lesion arises from within the marrow space, typically from the sphenoid or clivus. Classically, these lesions are lytic with expansile involvement of the diploic space on CT, often with thinning of both the inner and outer tables. They can demonstrate extraosseous extension. On MR imaging, there is reduced diffusivity and typically homogeneous, avid enhancement ( Fig. 4 ).
Plasmacytoma. Axial DWI images ( A ) demonstrate reduced diffusivity throughout the clivus. Axial T1-weighted images ( B ) and sagittal T2-weighted images ( F ) demonstrate the expansile nature of the lesion with corresponding CT images ( C ) depicting osseous destruction. Intermediate T2 signal is seen on T2-weighted images ( D ) with avid, homogeneous contrast enhancement ( E ).
Metastasis
Metastatic disease to the central skull base are less common compared to their intracranial counterparts. The most common underlying neoplasm to metastasize to the skull base is breast, followed by lung and prostate. Typically, these lesions are diagnosed in patients with known primary malignancies with evidence of metastatic disease elsewhere; however, in around 28% of cases, these lesions are the first sign of cancer. Headache, diplopia, or cranial nerve palsies in a patient with a history of malignancy should point the clinician toward this diagnosis. Imaging usually demonstrates either lytic or sclerotic lesions on CT with associated marrow replacement and enhancement following contrast administration on MR imaging ( Figs. 5 and 6 ).
Breast cancer metastases. Axial DWI images ( A ) demonstrate lesions throughout the calvarium demonstrating restricted diffusion. Coronal T1-weighted precontrast ( B ) and postcontrast ( C ) demonstrate corresponding enhancement with a dominant lesion of the frontal calvarium featuring intracranial/dural extension ( black and white arrowheads , respectively) . A lytic lesion involving the greater and lesser wings of sphenoid demonstrates osseous destruction on CT ( D, solid white arrow ) . T1-weighted images before ( E ) and after contrast ( F ) administration demonstrate extension along the middle cranial fossa and orbital apex ( dashed white arrow ). This patient presented with headache and symptoms of compressive optic neuropathy.
Urothelial carcinoma metastases. A 70 year old patient with no known primary malignancy presented with left sided visual symptoms. Axial CT images ( A ) demonstrate a lytic lesion centered within the anterior clinoid process ( white arrowhead ) . Axial ( B ) and coronal ( D ) T1-weighted images demonstrate loss of normal fatty marrow signal within the anterior clinoid process ( solid white arrows ) with evidence of corresponding avid enhancement following contrast administration ( C, E ) with extension into the optic nerve canal to directly involve the intracanalicular segment of the nerve ( solid black arrow ) .
Neoplasms arising from extraosseous structures
Nasopharyngeal Carcinoma
A relatively common neoplastic cause of skull base pathology originating outside of the osseous structures is that of nasopharyngeal carcinoma. There are 3 subtypes of nasopharyngeal carcinoma: keratinizing squamous cell carcinoma, nonkeratinizing squamous cell carcinoma, and poorly differentiated carcinoma. Often these tumors originate from the posterolateral pharyngeal recess, or fossa of Rosenmuller and appear as a soft tissue mass on CT. Of notable relevance to our topic, evaluation for surrounding osseous involvement is important. The American Joint Committee on Cancer tumor-node-metastasis staging system ninth version highlights unequivocal bony involvement as necessary for T3 category of staging, and therefore, the evaluation of underlying bone and skull base extension is paramount. MR imaging is often the optimal examination for complete evaluation of local involvement and perineural spread ( Figs. 7 and 8 ). These tumors typically demonstrate intermediate T2 signal and intermediate contrast-enhancement relative to the surrounding normal enhancing mucosal tissue. A key diagnostic feature on CT or MR imaging is that of soft tissue asymmetry/distortion relative to the contralateral side. ,